pgs. 8-23.doc
Treatment of Individuals with HIV Infection At Herdecke Hospital
Experiences, Hypotheses, Treatment Strategies (Original title: Behandlung von HIV-Betroffenen im Gemeinschaftskrankenhaus Herdecke. Merkurstab 1995; 48: 217-31. Record of a lecture (Medica, Stuttgart 18 Nov. 1994). The record
has been extended and an introduction added. English by A. R. Meuss, FIL, MTA.)
Christof Schnuerer
JAM Vol. 12, Nr. 3
Abstract
From 1985 to Jan. 1995 a total of 117 HIV and AIDS patients (265 admissions)
received inpadent care at Herdecke Community Hospital (HCH). Primary
reason for admission was, with few exceptions, advanced stage of the disease
(> B/2 in current CDC classification). Selected data of a retrospective analysis
covering 70 patients treated between 3/87 and 11/92 are presented and discussed.
The conclusions drawn from our material are considered in relation to
the current status of AIDS research, after which the question is considered:
how disease may be defined in terms of interaction between pathogen
(external factor) and host (self determination). An attempt is made to reduce
the many different conditions of human life to basic phenomena, one of these
being polarity and the balance created between extremes. Polar phenomena
can be perceived at different levels of life (micro, meta and macro levels). A
polar phenomenon at the meta level, the functional threefold order of the
human organism, first established by R. Steiner, is considered in some detail.
AIDS is then considered from this point of view, with treatment strategies
derived. Taking this approach further, critical questions arise concerning
chemotherapy, which is widely used to prevent opportunistic infections.
1. Introduction
The appearance of AIDS went hand in hand with a change in paradigm in
Medicine(1) which was not entirely triggered, but certainly catalyzed, by AIDS.
The "new disease" therefore marked a turning point in the history of medicine.
Pathophysiology is quietly leaving its classic models behind (e.g. Koch's
postulates and Virchow's cellular pathology) and becoming a science of "messages". "Communication" or, rather, "failure of communication" between
cells is the level where disease originates according to present ideas. Interest
now focuses on information transmitters (messenger compounds, cytokines).
The disease model is, thus, coming close to the "composition of bodily
fluids" again, though in the new way, and we have a kind of synthesis of
humeral and cellular pathology.
This approach will (need to) advance from the organization idea to one
of organism, with the latter taken as a purely spiritual concept. Leaving the
spirit out of account in medical research - which has been done most successfully
over the last 100 years - is reaching its limits in psychoneurotmmunology
today and in investigations concerning quality of life and coping with
illness. Primarily coming from the field of oncology, the above-mentioned
questions are coming up everywhere in medicine and have been given a new
dimension with the AIDS issue.
These are milestones on the road from thinking in a single dimension to
using more complex approaches. Man is increasingly seen as a multifarious
entity whose state of health or disease reflects concurrent processes and
relationships between different levels of existence. Anthroposophic medicine
offers both an anthropologic model ("Anthroposophy") and practical
methods and processes that can be followed.
Other attempts to develop a model of the human being that is closer to
reality than the somatic model are far less comprehensive. Thus the
biospychosocial model - to mention an approach that is widely accepted in
the Anglo-Saxon world - has been called "metaphysics without method,"(2)
among other things because of its inadequate anthropologic background.
(Another, more descriptive, way would be to say it lacks a real image of
man). This clinical model, introduced by Engel in 1977,(3) claims to be holistic
and seeks to include the psychologic and social levels in treatment, making
them equal to the somatic level.
Considering these developments we may say that in various respects the
spirit of the age in medicine has come closer than ever before to the
anthroposophic approach. This may be taken as an opportunity and, indeed,
a challenge to anthroposophic practitioners. It is important to realize that
AIDS acts as an indicator in this context, and the subject needs to be taken up
on a broad scale.
Below an attempt is made to develop a treatment strategy for HIV and
AIDS patients. It is published with the aim of contributing to the discussion
rather than offering a systematic or exhaustive study of the subject. Nor is it
intended to report clinical results but primarily to present a method and the
experiences on which it is based.
It is important to note that this is a record of a lecture given as part of a
training course in anthroposophic medicine (emphasis on threefold nature).
Simplification, where it occurs, was designed to meet the needs of the target
group. These passages have nevertheless been largely left unchanged, partly
for didactic reasons.
2. Clinical Background: Data and Conclusions
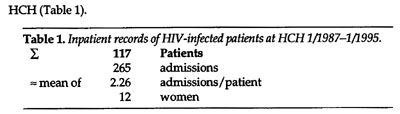
Between 3/87 and 1/95, a total of 117 HIV-infected patients were admitted to
The case records of inpatients treated from 3/87 to 1 Dec. 1992 (n = 70)
were analyzed in 1993. Selected data are given in Tables 2 and 3 and Fig. 1.
(Full documentation and two individual case studies have been published
elsewhere).(4)
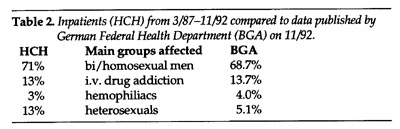
Distribution between affected groups (Table 2) in our material agreed
largely with that given by the German Federal Department of Health (BGA).
The same applies to age (36 years on average) and sex distribution.
Three differences should be noted, however:
1. The proportion of heterosexuals is distinctly higher in our sample.
2. The percentage of physicians (almost 8%, incl. one wife) is no doubt
higher than usual.
3. A proportion of 71% of supraregional patients (compared to 45% in
the rest of the department) seems worth noting.
Points 2 and 3 in particular suggest an atypical collective (special motivation?);
the trend in recent years has been a definite increase in regional
patients.
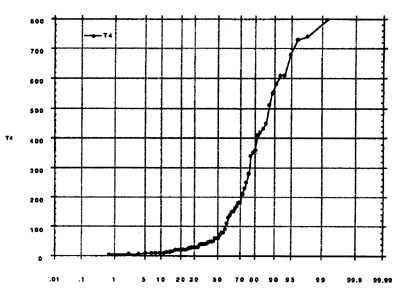
On first admission, immunosuppression was generally at an advanced
stage, with T4 levels below 200/pl in 70% (Fig. 1). This marks the threshold for
routine prevention of opportunistic infections. According to the American
CDC definition (valid from 1 Jan. 1993 but not adopted in Europe), this stage is
classified under AIDS irrespective of whether an indicator disease is present.
Table 3 correlates the mean T4 cell count on admission with survival time.
It seems appropriate to comment on the relatively high proportion of
patients who died during their inpatient period (7.1%). All of them died in
the first 3 years of the period under investigation (3/87-11/92). Since then
(until 1/95) we have merely lost one more patient on first admission, and that
was in 8/93. The reduction in deaths on first admission is no doubt partly
due to growing personal and general experience with AIDS (better range of
treatments and management).
However, the selection of patients clearly had a major influence. Initially
we admitted many patients who had largely been through all possible
treatments and were in the terminal stage (3/5 of the deaths on first
admission). Another patient consistently refused all active treatment, wanting
only nursing care and human concern. One single patient with previously
untreated acute AIDS and hemiparesis was profoundly unconscious on
admission and died before diagnosis and treatment could be instituted. In
retrospect, the rapid fatal end might perhaps have been prevented by
immediately initiating the established high-dose treatment for toxoplasmosis
(post-mortem examination was not possible). We were particularly affected
by the above-mentioned fatal outcome (8/93). After a cholecystectomy the
patient developed various mental disorders of a psychotic, catatonic and
depressive nature. He had previously shown depressive tendencies and was
under great stress psychosocially, and in the absence of other neurological or
MRI findings the changes were interpreted as a reactive psychosis. Shortly
before referral to the medical department (for further diagnosis and treatment)
he unexpectedly went into cardiac arrest, and following reanimation
survived for only a few hours. Histology of the brain showed diffuse cryptococcal encephalitis.
The case is described in such detail because it illustrates two basic problems
in the treatment of HIV infections: (1) the diagnostic problem (established
diagnostic criteria do not apply) and (2) a complex of neurologic,
psychiatric and psychosocial intentional factors that may result in signs and
symptoms being misread.
Our analyses agreed with the literature in showing a statistical connection
between life expectancy and mean CD4 receptor-positive cell count.
More careful weighting did, however, show the predictive CD4 cell
count to be absolutely unreliable in the individual case. Thus, we saw
unexpectedly unfavorable development even with high T4 cells counts (e.g.
510, with 26 months survival). On the other hand, relatively long survival
went hand in hand with low initial counts (e.g. 70, with 36 months survival).
Since the 9th International AIDS Congress in Berlin (1993), if not before,
the phenomenon of often highly individual developments has been widely
discussed as an important research issue. Interest focuses particularly on the
conditions for "long-term survival" of people with HIV infection. (The
definition of "long-term survival" in the literature varies).(5) Definition is,
however, of secondary importance in the present context, so there is no need
to go into it in detail.
More recent studies (e.g.(6)) appear to contradict the assumptions of earlier
studies (e.g.(7,8)) and show that lifestyle, coping, anxiety and depression do not
influence survival to the extent formerly assumed. Our observations have
shown, however, that rapid progression was often connected with negative
events in life (e.g. death of partner) and psychosocial stress (e.g. at work or at
home). Conversely, we saw the condition stabilize if it proved possible to
establish a stable therapeutic relationship and/or if psychosocial stress was
reduced.
Our conclusions agree with those published by Fauci in Science in 1993
after more than 10 years of intensive world-wide AIDS research:(9) AIDS is
more than just HIV infection.
AIDS is the consequence of a complex relationship between a person and
environmental factors in the widest possible sense. The how and why of the
relationship, from "transmission" to clinical manifestation, are conditions
that have now been largely followed statistically, but their "nature", original
causes and evolution essentially still need to be described.
Reduced to its basic phenomena, AIDS is a process between an individual
(host) and (many and varied) external factors. One of these factors is
evidently connected with a "mineral-like" life form consisting of little more
than information (virus). If we want to go beyond mere observation, it must
be permissible to ask what this "entity" has to do with the human being.
The relationship is clearly intimate, for not only does the virus depend on
the human being for its survival (no animal model exists), but its information
structures are closely related to human genes, with its integuments more or
less a counter image of cell surfaces. Apart from anything else this entity has
possession of the "security key" to the human immune system. (Such a
process shows the close, complementary relationship between human and
world, casting doubt on the idea of "chance" triggering a disease, even from
the microscopic point of view).
The "pathogen" may almost be said to be intelligent and well informed
in the way it has adapted to the state of present knowledge, and is, therefore,
able to resist treatment. (In a similar context Dumke(10) quotes Adolf Portman
who, with reference to the pathogen causing rabies, speaks of the
"extraneous knowledge" held by microorganisms, calling such properties
"truly demonic"). Yet many of the factors which trigger disease are directly
or indirectly dependent on man (Table 4) and, therefore, open to treatment
strategies in the widest sense.
Which are the effective methods available today?
Prevention is acknowledged to be the most effective individual treatment for
AIDS. It depends entirely on the individual, however, on his behavior and
the way he deals with psychological conditions (desire for pleasure -
sexuality - addiction).
The experts generally agree that the world-wide struggle to deal with the
pandemic can only be won if the following "social diseases of our time" can
be limited:
1 Social imbalance (poverty on one hand and pointless riches on the
other, with disease rife at either extreme)
2 World-wide desolation in education systems
3 Epidemic spread of addictive structures.
The current situation forces us to consider the virus issue as secondary
when it comes to treatment. (Hopes of a vaccine that would really change the
situation are illusory; even if it were to be unexpectedly available in a few
years, it is unlikely to have any real effect on the evolution of the pandemic).
This point of view justifies the objections (raised by a number of authors,
P. Duesberg(11) in particular) to monocausal viral genesis or simplification of
causality. Duesberg's emphasis on drugs and medicaments as causal factors(12)
may then appear in its right light - on a different level, of course, from the
biased and simplistic views presented by virologists not familiar with the
clinical situation.
3. Initial Hypotheses for our own AIDS Strategy
Our own approach to research and treatment bases on the many indications
Rudolf Steiner gave concerning the outstanding role the host plays in
infection.(13)
Our analyses of causes and search for suitable treatments has, therefore,
always concentrated on the human being. In our approach to treatment we
were thus able to abandon the limiting view of viral origins and treat
antiviral strategies (e.g. AZT, DDI, DDC) with pragmatic and critical
distance. (This made it easier in the early days of AZT euphoria to base
ourselves on our own clinical experience with the substance and not just on
statistical successes reported with surrogate markers. More recent trials (e.g.
CONCORD) justify this approach).
In other words, we focused less on the microscopic causes and more on
the macroscopic phenomena. (Albonico asked for the HIV dogma to be
overcome(14) in a paper published in this journal in 1993. We concur with this,
certainly as far as the clinical aspect is concerned).
Here it becomes necessary to define our concepts and method.
Basic Concepts, Phenomenological Method
Human life can be described and defined in many ways, depending on our
point of view.
An important basic phenomenon is clearly that of constant change
(metabolism, development, transformation).
A person's current state of life (and health) is, therefore, a snapshot of a
complex developmental process which may be said to have three basic aspects:
1 somatization (physical biography) determined from outside
2 socialization (social biography) shaped by self and others
3 intention (intentional biography) self-determined
The physical biography is determined by conditions "typical" for all human
beings. Simplifying the matter we may speak of the human race being subject
to natural laws which include the laws of development and aging, genetic
aspects, laws governing the intake, transformation and elimination of matter.
This part of our biography is predetermined; it is determined from outside.
At the other extreme we have our intentional biography. This depends on
how we, as individuals, deal with our life. It is a self-determined act of freedom.
Between these two we live our social biography which is partly determined
from outside (e.g. nationality and gender) but is also partly shaped
and determined by ourselves; it lies between outside- and self-determination.
To avoid any misunderstanding let me say that these levels do, of course,
initially form an indivisible whole that can only be differentiated in our
thoughts. On closer consideration it also emerges that both in individual
development - depending on the age reached - and in human evolution the
balance between the three biographic aspects changes. This is clearly evident
in childhood (the intentional aspect is little developed, the middle region is
largely determined by the social environment; childhood diseases are, there-
fore, highly "typical" and subject to strict laws).
Human development, human life, is thus unthinkable without the field of
tension between outside- and self-determination. We may also call outside
determination the "supra-individual" aspect (typical, subject to natural laws,
generic). This part of the biography is largely determined, foreseeable and,
within limits, "calculable". The opposite extreme, the individual, self-
determined aspect of the human being is essentially creative, producing
things that are new, and therefore unforeseeable and "incalculable". (Modern
medical science is almost exclusively concerned with the calculable aspects of
human reality. This makes it so convincing as a science, for questions and
results relating to natural laws are usually repeatable).
The condition of "health" would thus be defined as: the individual's
ability to maintain the balance between the supra-individual (typical) and individual
(creative) aspects.
Conversely, the condition of "ill health" may be defined as: a shift in
balance towards the supra-individual, typical (which may be due to external or
internal natural laws). The more marked the shift, the more distinct
(textbook-like) the disease.
The middle region, the social environment, can balance an upset
equilibrium (a task for the art of healing, for instance) or increase it and,
therefore, favor disease.
"Medicinal" in this sense would be measures that enable a person to
maintain his individual nature, his intentions, in the face of the disease type.
Definitions should not block our view of the rich potential for variety in
the world. They can only present a partial aspect of the complex disease
phenomenon, an aspect, however, that would appear fruitful in the current
context.
4. Therapeutic approach between self- and outside determination
If we consider AIDS in the light of the above, it can be seen to be a characteristic example of evolution from individual to typical aspects ("de-individualization")
The disease begins in a variety of ways, being non-characteristic and
individual and becomes increasingly more typical and instantly
recognizable in its advanced stages. The approach to treatment results from
the above characterization of the disease. On one hand the individual pole
must be strengthened, and on the other the pole of external determination
must be forced back.
It is, of course, easy to formulate such a hypothesis. It needs to be made
specific for implementation. As a first step, let us consider certain aspects of
external determination in some detail.
External determination of AIDS pathology
It is "typical" of AIDS pathology (pathology in the fullest sense) that affected
individuals are subject to powerful external factors coming from two
directions as soon as they are known to be HIV positive.
This is the (allegedly) inevitable progression from "positive HIV test" to
AIDS and death, a route laid down - as the general message goes - by a life
form infesting the blood and subject to mathematical, statistical laws of time
and the pitiless dictates of laboratory parameters. The affected individual
feels inwardly taken hold of by a "foreign will". This fills him with
paralyzing fear and/or leads to evasion and repression strategies. Hopes for
the future narrow down to foreign substances (the feverishly sought AIDS
drug) and frequently suicide. Killing oneself thus becomes the ultimate
symbol of free decision and self-determination. (Usually planned for a long
time, suicide is often literally "celebrated" as driving the foreign element out
of the body and taking one's revenge on the natural laws governing the body,
laws not accessible to human intentionality).
The second factor is the "typical" reaction of others (including medical
personnel), which tend to isolate the individual and determine the affected
person's life from outside. Attitudes such as these arise from hysterical fear of
an entity not perceptible to the senses that treacherously seeks to attack and
destroy and only waits for an opportunity to invade. Defensive reactions are
enhanced by a tendency to "typify" those affected (assignment to groups,
moral judgment and condemnation). Absurdly enough this applies even to
children, irrespective of the route of transmission.
The social environment often becomes unbearable for the patient, with
the social biography entering into a vicious circle of fear, lies (a core problem
in AIDS pathology) and withdrawal. Paralyzing fear of the changes subject to
natural laws in one's own body, encounter with and lies from the social
environment are undoubtedly powerful external factors.
The therapeutic triad: removal of fear, activation and change
The first step, usually only partly achievable yet all the more important, is to
remove fear and free the individual from a narrow view of the future and the
world. It creates the precondition for the steps that follow.
Basic conditions for the resolution of fear are an open, fearless approach
and a social environment where people have awareness of the significance of
truthfulness. This alone will remove the fear of medicine and its institutions
and of unwanted diagnostic and therapeutic interventions. It provides the
soil in which "broadening" of the patient's view of the world can grow. With
new interest in the rich variety of the world, in nature, other people, and the
social environment, the frozen inner attitude is resolved. A horizon
previously reduced to an ominous virus, medicaments, symptoms and
laboratory results can expand.
The preconditions are created for activation of such resources as are still
extant. Avenues are opened up for something new and creative, elements
that can be freely shaped in one's own destiny. Self-awareness and awareness
of others, egotism and altruism can be brought into balance in a new way,
which the individual finds for himself, and, finally, the social constriction
also is resolved.
This is a process of change, with a disease tending towards constriction
and destruction "changed" into its positive counter image. It is overcome as
room is made for perception, insight and action, in spite, of, and indeed
because of, the disease.
The finite nature of (one's own) life can be accepted as a universal law
that has meaning and loses its will-paralyzing character. Limited periods of
time are given their relative value and lose the aspect of hopelessness. Here
and today, anything that can be done now becomes just as important as the
future which, in the final instance, is limited for every human being. The
utterly individual "melody of life" (what do I want to find in life, what
meaning do I give to life) can be intuited and - in all modesty and with love
for its imperfections - so that it begins to sing.
Change as an actual treatment goal means that the individual consciously
addresses his development potential. Change and development, rather than
standing still and paralysis, are the laws of life processes, and the process of
change can take effect even at the level of physical functions.
Change is ultimately the ability to gain a new balance between natural
laws at one extreme and intentionality at the other. The condition has been
reached which was defined as "health" above, though in a sense it differs
from the generally accepted. Here the concept of health becomes free from
defined physical parameters (e.g. laboratory results). The latter become mere
indicators that may point to the balance being threatened.
It is also possible to say to one's patient:
The disease does, of course, have aspects where it is subject to natural laws.
This may be denned by reference to a virus, if one wishes, with figures and
statistics used to define the type.
Human beings also have another aspect, however, which is individuality,
intentionality and creativity. This determines the course the disease
takes just as much as the laws of nature do. It is also possible to speak - to
anyone prepared to listen - in terms of the field of tension between determination
from outside and self-determination. This is the absolutely essential
driving force for human development. Potential energies grow as the tension
between the extremes increases. This is the tremendous challenge AIDS
presents with its undoubtedly powerful aspect of outside determination. At
the same time it is an enormous opportunity for development.
Importance of art therapies
Removal of fear, activation of inherent potential and change are processes
that cannot happen unless great efforts are made to come to terms with
oneself. Help and support will be needed from others (therapists). It will only
rarely be possible to be consistent in following this path, for in many respects
we lack the preconditions for this today. Yet - as our experience has shown -
the therapist should not let this realization stop him from setting out on the
path. Individual steps and partial results are also helpful.
Pharmaceutical substances should only be used for limited periods if
possible, essentially as a prosthesis in crisis situations. Art therapies are the
appropriate aids on the road to removal of fear, activation and change. They
are material (modeling, painting) and immaterial (music, speech, poetry,
eurythmy) "medicines" and serve to transmit a message from one person to
another.
The therapist becomes the medicine, the quality of which depends entirely
on his human and professional abilities (training - schooling).
Change as an extended form of rehabilitation
Change as the real treatment goal is undoubtedly related to rehabilitation,
but we have chosen to use the term in an extended and specially-defined
sense. It is not a question of "returning to the conditions that existed prior to
the illness", as the term "rehabilitation" suggests. The "old conditions" did,
after all, lead to the illness. The road which led to loss of balance must be
abandoned and a new road found that leads to a new state of balance.
This is no doubt one of the most difficult messages in our approach to
treatment, and many patients are unable to accept it or can accept only some
of it. It (apparently) contradicts the strategies generally proposed today,
where the goal is to maintain the usual life style for as long as possible. This,
of course, is in reality quite impossible, for thoughts of the disease,
symptoms, the need to take medicines, etc. change the individual's lifestyle
quite considerably.
We must be careful not to impose our own views on the patient. They
can only be presented when aspects such as these have become part of the
patient's experience. It would go against the stated goal of strengthening the
self-determination pole if a therapist sought to impose his own system and
thus determine from outside.
5. Polarity at the Different Phenomenological Levels
Above, the polarity between supra-individual and individual aspects was said to
be the driving force in human development. I would call this a polarity on the
macro level. (This is even more so the case with the polarity between spirit
and body). The question is: how far can the principle of polar forces also be seen
at other phenomenological levels of life and utilized for therapeutic purposes?
It is easy to see polarity as the basic condition for life at the micro level
when considering the membrane potential of cells, for instance. Here
permanent loss of polar tension is identical with death. The theme of agonist
and antagonist of messenger substances, which occurs in countless
variations, also shows the polar principle. Medicine works on this level today
when imbalances are corrected by substitution or inhibition.
Can the principle also be found at the meta level?
Functional polarity in the human body
Rudolf Steiner's researches led him to recognize two polar functional
principles in the human organization as a whole: the neurosensory sphere on
one hand, and the sphere of metabolism and limbs on the other.
Simplifying the issue, we may also speak of polarity between the upper
and lower human being. (This is, of course, schematic and may cause
misunderstanding, but initially it is helpful in thinking things through.) In
the head, the upper human being, the neurosensory process is functionally
dominant (not exclusively so); below the diaphragm, in the lower human
being, metabolism determines function (though again not exclusively so). The
fundamental differences are easily brought to mind if a phenomenological
approach is used.
If we take this further, we realize that catabolism dominates in the upper,
and anabolism in the lower human being. Processes dealing with imponderables
(sensory impressions) are also mainly in the upper human being,
those dealing with physical matter (digestion) in the lower.
This functional tension is balanced and mediated in the middle human
being, in the rhythms of the pulsating blood and of respiration. Phenomenologically,
seen in terms of the density and weight of matter, respiration is
beyond the solid and fluid elements we have in digestion; yet, on the other
hand, it is more material than our imponderable sensory impressions.
The middle position of the thorax can also be seen in the skeleton.
Endoskeleton in the sphere of metabolism and limbs, exoskeleton in the
region of the head, and in the thoracic region a rhythmic exoskeleton (the rib
theme recurring and fading away) that gradually dissolves lower down.
Here we have a functional threefoldness of the organism, with the tension
between extremes the driving force.
Thinking in analogies - a useful method?
The above may be seen as a pretty analogy and accepted or rejected as such.
Yet what matters is whether this approach can be used to develop useful
ideas for treatment.
If we consider HIV infection from this point of view, we realize that its
primary manifestation is in all three functional spheres.
If the question as to where AIDS-defining pathology finds its location is
seen not as chance exposure to a pathogen (i.e. statistical risk relative to CD4
cell count), but functional dispositions are also taken into account, our
treatment strategies will differ from those generally used.
It then becomes justifiable to ask why one person first develops pneumonia
(middle human being), for instance, another severe diarrhea (lower
human being) and a third an opportunistic infection of the central nervous
system (upper human being), and why in an individual case the pneumonia
is followed by diarrhea or toxoplasmic encephalitis. Is this chance or can an
inner (polar) connection be found between these events?
We noted that tendencies to diarrhea and severe cerebral manifestations
are interrelated in that people with cerebral disease do not usually develop diarrhea and, in fact, are not infrequently suffering from persistent constipation.
Alternation in time is another feature. Recently, we had a patient with
severe nonspecific diarrhea who would develop focal seizures as soon as his
diarrhea stopped. The hypothesis we have evolved from this is that the above
manifestations show alternation between the opposite poles in the human
being that were discussed above. We are, therefore, always on the lookout for
early neurological signs in patients with persistent constipation and will take
preventive action where indicated, using (saline!) laxatives. It will require
further investigation to see if this measure will actually reduce the frequency
and severity of cerebral events.
Symptoms - indications of counter-regulatory reactions?
This raises questions which may be of considerable clinical import:
Can symptoms in one functional sphere of the organism be signs of
counter-regulatory reactions at the other extreme? Also, could it be that
exhibition of prophylactic antibiological agents (currently the major strategy
to prevent opportunistic infections) favors manifestations of a different kind
in another site?
Figures for the evolution of opportunistic infections over the last 6 years
published by the German Federal Department of Health(15) would, in my
opinion, fit in with the hypothesis. Thus the incidence of Pneumocystis carinii
pneumonia (PCP) showed a distinct reduction (by almost 20%) with preventive
treatment (mainly pentamidine), but the incidence of opportunistic
infections has been rising steadily (from 67% in 1987 to 72.4% between
7/1993 and 6/1994). The main infections have been toxoplasmosis, which is
more difficult to treat, CMV infection with its wide range of manifestations,
and typical and atypical mycobacterial infections.
I am familiar with the objections which are raised: the last-named
opportunistic infections only manifest with low CD4 cell counts (less than 50-
100 /ul). From this point of view, it is due to PCP prophylaxis that more of
those affected experience the more advanced stages of the disease. In my
view, these are important considerations but not proof for they base merely
on surrogate markers such as the CD4 cell count.
Multiple prophylaxis used to treat statistical risks
It would go too far at this point to discuss all the pros and cons of relatively
broad-spectrum antibiotic prophylaxis to prevent opportunistic infections
with HIV syndrome.
At the least, statistically demonstrable reduction in infection should not,
in itself, be considered adequate justification for the widespread use of
powerful drugs with numerous potential side effects. The likelihood of
resistance developing, the negative effect of exposure to resistant pathogens
and substances with uncertain long-term toxicology, both on the individual
and on subsequent patients, must be taken into account just as much as the
possible extension and quality of life.
It seems to me it would be more intelligent for anyone who feels it
necessary to pursue such a strategy to use specific prevention or perhaps
treatment, establishing a risk profile for the individual patient. Points of view
such as those given above concerning the threefold organization of the
human being may prove helpful in this and should be explored.
It also seems to me that qualitative aspects are left aside in the discussion of
broad-based prevention (5-fold prophylaxis is not uncommon today). To
mention just one: can a primary manifestation such as pneumonia have
positive effects at another level of the human defense system?
On several occasions we have seen patients who had overcome PCP
(So far no PCP with fatal outcome at our hospital.)
gain a different attitude to their disease and, hence, an opportunity to use
their resources.
After the pneumonia I actually realized that I have to be active myself and
started to make something of the time which is available to me. I started to
live.
This is an important basic issue in the treatment of AIDS. Our present
view is: instead of a schematic strategy dependent on numerical values the
atm is to develop an individual risk profile for each patient which covers
physical aspects (weak points, prior problems, dispositions) as much as
intentional potential (active prevention, e.g. with art therapies), the social
network (social support) and psychological conditions (fear and anxiety,
repression).
Much research clearly still has to be done; the benefit of such research
would, however, greatly outweigh the cost if positive results could be
achieved. An additional gain would be made not only in quality of life for the
patient but also in reduced financial expenditure, doubtless with greater
need for human resources. Our clinical experience to date would seem to
bear this out.
6. Schematic Review of Treatment Strategies
1 Considering the human being in terms of processes in polar fields of tension at
three levels:
Biographic (mega level)
Organismal and functional (meta level)
Fine material, cellular (micro level)
2 Therapeutic steps at the mega and meta levels
Art therapies, biography work and process-activating medical treatment
Removal of fear
Personal activation
Change
3 Intervention on micro level if balance can no longer be maintained ("pros-
thetic function")
Supporting material and processual balances with substances and
medicaments
Suppressing foreign processes (e.g. antibiotics, virostatics, antimycotics).
Christof Schnuerer, MD
Geineinschaftskrankenhaus Herdecke
Beckweg 4
D-58313 Herdecke
Germany
References
1 Marcus U. Paradigmenwechsel, Symbole und neue Wege der Problemloesung. AIDS and HIV-Infektion, H. Jaeger (ed.) 1992; 10. Erg.-Lfg 4/93.
2 Sadler J, Hulgus Y. Knowing, valuing, acting: Clues to revising the biopsychosodal model. Comprehensive Psychiatry 1990; 31:185-95.
3 Engel G. The need for a new medical model: A challenge for biomedicine. Science 1977; 196: 129-36.
4 Schnuerer C, Aldridge D, Altmaier M, Kleinrath U, Neugebauer L. Kreativitaet, Individualitaet - Wege in der AIDS Therapie: AIDS Forschung (ATO) 1995; 15-35.
5 Keet R, Krol A, Coutinho RA. Long term asymptomatic HIV infection. Muenchner AIDS-Tage Jaeger H (ed.) 1994; 80-81; Landsberg/Lech: ecomed.
6 Kessler RC et al. Stressful hfe events and symptom onset in HIV infection. Am J Psychiatry 1991; 148:733-8.
7 Blaney N et al. A stress-moderator model of distress in early HTV-1 infection: Concurrent analysis of life events, hardiness and sodal support. J Psychosom Res 1991; 35:297-305.
8 Catalan J, Klimes I, Day A, Garrod A, Bond A, Gallwey J. The Psychosocial Impact of HIV Infection in Gay Men - A Controlled Investigation and Factors Associated with Psychiatric Morbidity. Br / Psychiatry 1992; 161: 774-8.
9 Faud AS. Mulrifactorial nature of human immunodefidency virus disease: Implications for therapy. Science 1993; 262:1011-18.
10 Dumke K. AIDS: The Deadly Seed. Tr. C. v. Amim. London: Rudolf Steiner Press.
11 Duesberg P. HIV and AIDS. Science 1993; 260:1705.
12 Duesberg P. Can Epidemiology Determine Whether Drugs or HIV Cause AIDS? AIFO 1993; 627-35.
13 Steiner R. Spiritual Science and Medicine (GA 312) lectures of 22 & 24 Mar 1920. Tr. not known. London: Rudolf Steiner Press 1975.
14 Albonico H. Die Ueberwindung des HIV-Dogmas: Ansaetze zu einer erweiterten Sicht von AIDS. Merkurstab 1993; 46:59-63.
15 Robert Koch-Institut, AIDS-Zentrum. AIDS/HIV: Quartalsbericht 11/1994. 114. Bericht; Berlin 1994.