pgs. 57-75.doc
A Patients Biography As An Aid to Diagnosis and Therapy:
Research at Klinik Oeschelbronn (Original title: Die Krankenbiographie als diagnostisches und therapeutisches Element.
Merkurstab 1995; 48:177-92. English by J. Collis, MIL.)
Hans Werner, Elke E. von Laue, Hans Broder von Laue
Introduction
Cancer is a disease of the present time. It creates an atmosphere of fear that
makes specific demands on patients, their environment and care providers.
Physically it causes chaos in the morphology. As far as vitality is concerned it
manifests as unchecked cell growth. Psychologically it opens the door to fears
and feelings of hatred. Spiritually it can be a consequence of lacking self-development and failure to shape one's biography. The latter does not apply
to childhood malignancies. Although cancer follows certain patterns, the
course it takes is as individual as any human biography.
Physicians have to regard cure as the goal of treatment even when the
stage the disease has reached takes them to the limit of their courage. The
more they feel that their courage and will to heal can be effective even
beyond death, the more will they be able to help. To assess the efficacy of
treatment as a whole it can be useful to make a prognosis based on the
patient's clinical condition and state of mind before treatment begins. During
treatment the prognosis and actual progress of the patient are regularly
compared.
A number of organism- and tumor-specific parameters have to be
considered for assessment of results. For the purposes of this paper the
patient's general health and temperature will be the organism-specific
parameter, and the growth rate of pulmonary metastases the tumor-specific
parameter. We are aware a more differentiated approach may be used but
have limited ourselves to these two for the purposes of this paper. The
diagnostic and clinical value of eurythmy therapy given at intervals during
the whole course of the illness is also considered.
A biography takes shape in time as it unfolds between birth and death.
The resulting shape is not an object to be discerned with the senses. It
develops over time and arises from the qualities of time - past, present and
future. A biography can only be seen inwardly as the panorama of a life if we
concentrate on crystallizing out the sequence of experiences and events. From
prenatal obscurity every individual brings gifts that may hinder or help.
Through a series of metamorphoses governed by specific laws, physical
organs as well as mental and spiritual faculties are developed as these gifts
interact with external circumstances and events. Capabilities can be used to
shape one's sphere of life and to realize ideals and aims. Every human
biography is unique since the variety of given and added inner and outer
possibilities is so enormous that no life is the same. Yet every biography is
founded on a generally valid human blueprint that is modified by personal
and suprapersonal influences.
An attitude of reverent reserve and the greatest tact are prerequisites for
working with the biography of a sick individual. With practice we can
develop faculties that allow us to discern more and more clearly the many
and varied interconnections and developments in a life. Understanding what
has led to the present life situation of the individual we may be able to draw
conclusions as to what might "turn the situation round" in the future. Below,
an attempt is made to demonstrate the possibilities that arise out of working
with a patient's medical biography. The patient gave her consent.
The Biography - (P. R.)
Stooping slightly, the slender 60-year-old woman came into my consulting
room, moving more slowly than normal. Skin pigmentation was increased so
that the pallor was reduced. She had rings round her eyes. Her expression
alternated between quiet sadness and moderate vivacity. Initially she didn't find
it easy to talk about her life, but her confidence gradually increased over several
talks, and as time went on the periods she had left blank began to fill in.
18 months earlier, Mrs. R. had noted changes in her right breast. Having
taken early retirement, she was working as a supply teacher in schools and
had used this as an excuse to put off going to the doctor. The changes became
more marked after 18 months, and she finally decided to see a doctor. On
operation it was evident that the cancer had spread to the regional lymph
nodes and established multiple lung metastases.
1st to 21st Year
First 7-year period. The family was middle-class. The birth was 10 days late
and required forceps delivery. Her mother had sufficient milk and breast-fed
her until the family doctor, noticing she was becoming exhausted, advised
that the baby be weaned rapidly. Her mother was dutiful by nature and
permanently over-burdened because, apart from her own household, she
helped out in her parents' bakery in a rural district. She was unable to give
her child the necessary warmth. The patient's father was a customs official.
He was stem, proud and domineering. Obedience was his chief requirement,
and the daughter obeyed without resisting. Remaining within the bounds he
imposed she experienced her father's caring love in a special way. No siblings
were born. At 5 she had measles that did not manifest properly and were said
to have weakened her eyesight. She started school at 6. Shortly before the end
of her 7th year she had an experience that affected her deeply. This was at
Christmas. Entering the room where the Christmas tree stood she saw a dolls'
pram under the tree. She had longed passionately for this pram and ran
towards it with cries of delight. In doing so she forgot her father's stem
commandments and had to be punished for upsetting the customary Christmas
evening procedure. The pram disappeared and was never given to her.
Second 7-year period began with another profound experience. Her father
died of a heart attack when she was 9. Loneliness now crept into her life. She
felt as if she had been deserted, and an immense sadness grew in her. She had
diphtheria in the same year. She found her mother a generous person, but
unapproachable and hard. She described herself as having been a quiet child
who spoke little and lacked cheerfulness and gaiety. She sensed her mother's
disappointment. At 12 she began to keep a diary which she filled with her
longings, hopes and poems. She sought recognition and praise at school
because she couldn't expect them from her mother. Apart from this she felt
disadvantaged and stupid. She only did well with teachers who recognized
her worth. She developed mumps at age 12. This was also when she began to
have digestive problems that accompanied her throughout most of her life,
and a postural weakness of the spine. Her periods began at age 13 but
remained very irregular until she was 15.
Her melancholic mood and retiring nature increased her sense of
isolation during the first half of her third 7-year period. She passed her school-
leaving exams at 18. This was followed by compulsory community service
when she consciously experienced companionship for the first time. She
wanted to study biology, but this was not possible towards the end of the
war, and she took a one-year training at a teacher training college. In the
chaos of the final war months she worked first as a teacher and then as
forewoman in an aircraft factory. At 21, she experienced the terrible
consequences of a heavy bombing raid on her home town.
21st to 42nd Year
Separation from her mother came at the beginning of her fourth 7-year period.
The parting was not easy, and she developed a serious attack of hepatitis at
the time. Commuting daily to her new job she met a teacher who knew a
great deal about science, languages and music. Life grew very intense and
she became engaged to him. However, she was unable to cope with the high
degree of mental stimulation he gave her, and contracted recurrent bilateral
pyelonephritis at age 24. She became increasingly exhausted and finally had
a complete breakdown at 27. She parted from her fiance.
At the beginning of her fifth 7-year period she was called to join the staff of
a teacher training college. This was the beginning of a hard, difficult, busy
and successful time. She met a woman who became a life-long friend, in the
middle of her 32nd year she had a profound, never-to-be-forgotten friendship
with a man.
Her sixth 7-year period began with the abrupt ending of this relationship.
A year later, against the advice of friends, she decided to marry a widower
with 3 children. She got on well with her step-children and experienced the
joys of motherhood at 39 when her only daughter was born, a forceps birth.
She gave all her love to this child, endeavoring to give her all the things she
had lacked in her own childhood. Her husband was an officer, and the
marriage was difficult. The partners had widely differing interests. Her
mother-in-law's behavior and a powerful bond between her husband and his
mother brought discord into their life. Hostilities increased and led to
tensions that burdened the couple's relationship. Having kept her full
professional life going in addition to running the home she became totally
over-burdened. She took refuge in her professional work.
She didn't want to talk about the next two 7-year periods leading up to
her 56th year. A drawing she made showed a long succession of high points
and successes in her school work in contrast to repeated psychological
disasters in her marriage. Parallel with these psychological difficulties, after
her 42nd year she suffered increasingly from cardiovascular disease and
gastrotntestinal problems that undermined her strength more and more.
From her 51st year onwards the psychological tensions increased. In
connection with the menopause she repeatedly suffered from exhaustion and
started to have sciatica and migraine attacks. For this reason she took early
retirement at the age of 56.
She got on well with her daughter until she turned 16, when difficulties
began. The daughter criticized her, and she realized from talks with her that
she had brought her up with too much "love", having lacked love in her own
childhood and youth. She awoke from an illusion and felt a return of the
inner emptiness and sense of desertion that had accompanied her youth.
Similarities between daughter and husband also opened her eyes to the
various actions and reactions of the latter.
When she was 59 she discovered the changes in her right breast.
Roots of the Illness
If we can succeed in forming a picture of a biography and then compare this
individual life with the general course of human biography and the
underlying laws of metamorphosis, we can begin to understand how
illnesses arise or become tendencies. People today find it difficult to
understand the language of inner destiny (gifts and dispositions brought into
life by the individual) and outer destiny (events and encounters). One of the
physician's tasks needing great tact and sensitivity is to help a patient
decipher this language.
The child was born with the aid of forceps, and 10 days late. The rigid
up-bringing by a stem and domineering father combined with the mother's
dutiful attitude and lack of warmth were not likely to encourage the
approaching ego's will to incarnate. The weakness in incarnating was most
probably also further enhanced by that deeply-felt, painful experience at
Christmas. Childhood diseases are an expression of the ego's efforts to mold
the inherited model body. An attack of measles that did not fully develop
and the relatively late attack of mumps are probably signs of a weakened
ego-constitution. During this period of life the growing individual is a
creature of movement living in imitation, with the organs developed and
brought to maturity by factors coming from outside. Is it not possible to
imagine that the limits set to manifestations and enjoyment of life by the stern
up-bringing and lack of maternal warmth might have affected the quality of
the developing body? Conversely, the body is an instrument spirit and soul
use in coping with life and shaping its course. Thus the developmental goal
of the first 7 years was not quite reached, resulting in some degree of
retardation.
During her second 7-year period the patient was withdrawn and quiet,
lacking the gaiety and capacity for sympathy of this age-group. She
blossomed and was able to express herself, however, if treated with
understanding and appreciation. Her mental disposition was reinforced by
the death of her father, whom she loved despite his sternness. She missed the
authority of which she had stood in awe, and there was no longer any
compensation for her cool mother's lack of understanding. She inevitably
succumbed to melancholic states, withdrew into herself and wasn't able to
gain sufficient experience of, or practice in, the breathing of the soul that is so
important as life proceeds. The result was an asthenic constitution and the
onset of digestive problems and postural weakness, also the expression of the
ego's failure to take a firm hold of the body at this age, when it approaches
via the metabolic system and the limbs. Menstruation began at 13 but her
periods remained highly irregular for 2 years, with full earthly maturity not
attained until 16.
Earthly maturity, the achievement of one's own rhythms, the adoption of
the body by the ego, and gender-specific development are all prerequisites
for breaking the ties of heredity. This opens the way to development of one's
own life of feeling and will, and thus to I-You relationships. The patient had
developed a feeling life of her own from the age of 12, which is rather early.
However, this remained entirely inward, and she had little contact with
others. Symptoms in her physical development point to forces being held
back that ought to be available for inner development during the third 7-year
period, but she remained withdrawn and friendless during this period. She
related only to teachers who showed understanding and appreciation. The
final third of this period was marked by school-leaving exams, her first
experience of companionship during community service, frustrated choice of
profession, the chaos at the end of the war, emergency training at the
teachers' college, being overtaxed by immediate full responsibility as a
teacher, fleeing the approaching enemy troops and experiencing the
catastrophic destruction of her home town. The war situation had
temporarily removed her from dependence on her mother.
Did she achieve the aim of this period - responsibility in forming her
own judgments and carrying out her own actions? We find the answer in her
fourth 7-year period. She described it as a time when she had profound
encounters and had difficulty in becoming independent of her mother. She
became at home in her profession. Her first serious encounter with a member
of the opposite sex led to illness, exhaustion and finally a breakdown because
it overtaxed her mentally. She broke off her engagement at the age of 27.
The kidneys are the main organs for developing the sentient soul during
this period. But the sentient soul was not entirely able to cope with the many
different phenomena and human encounters. The patient "mastered" her
profession but not the I-You relationship. Did soul forces not transformed by
the ego have a pathological effect on her kidneys? She did not quite manage
to achieve the developmental goal of the fourth 7-year period that is typical for
the human being in general.
The fifth 7-year period is the middle of life and in her case brought the
most important human encounters. In her 30th year she got to know a female
colleague with whom she shared interests and holidays. They parted only for
professional reasons at the time when she married. Inwardly they remained
connected for life. Between 32 and 36 she had the indelible experience with a
man. This ended abruptly and left her with a permanent sense of longing.
As though under a compulsion and almost without thinking things
through she decided to marry in her sixth 7-year period at the age of 37. She did
not want to miss out on the joy of being a mother and found it in the
motherly care she lavished on her 3 step-children and the affection that came
to her from them. Her own motherhood came as a climax in an otherwise not
very happy private life. Tensions and conflict had already begun in her
marriage and were not to end until her death.
The subsequent 7-year periods until she became ill show how her ego failed
to master life's problems. The aging process started early and showed in
cardiovascular disorders, gastrointestinal problems, and sciatica. She had to
give up her profession, which was her elixir of life, at 56. Her profession had
always been the mainstay of her life, enabling her to maintain her self-esteem
through the recognition it brought her. Within the family she had drawn self-
esteem solely from the intimate relationship with her own child. But this
illusory support was taken away from her. Just as had happened after her
father's sudden death, emptiness, despair and inner loneliness once more
took hold of her inner life. Then the tumor made its appearance.
Like a thread running through the first half of her life we have the
impression that the metamorphoses of the 7-year periods were not entirely
successful but generally somewhat delayed. Her physical body was born late
and only with mechanical help. The birth of her life body was somewhat
delayed, which meant she was not quite ready for school. Earthly maturity
was also delayed. The birth of her ego was not entirely successful, as is
shown particularly in the failed I-You relationship in her fourth 7-year period
and by the hepatitis she suffered in her 22nd year. Did the ego fail to develop
a sufficiently healthy bodily constitution and to transform the formative
forces of the soul as they became free in the 7-year stages so they could work
on shaping her life? Had her body, soul and ego been too weak to cope
sufficiently with the demands made in the second half of her life?
The second half of her life shows how the tendency to be retarded in the
first half of life changed into an accelerating process in the second half. The
aging processes entered too early and too deeply into the physiology. They
forced the ego-organization away from its task of restricting disorderly
growth, giving shape to the body and preserving it. The cardiovascular
disorders, gastrointestinal problems, sciatica and states of exhaustion were
reflections of this in body and soul. The ego failed to master the family
problems, and the unused soul forces turned on her body instead. In this
sense the physical and psychological illnesses that had been developing since
her 42nd year were an expression of functional carcinosis, indicating a
general disposition to cancer.
Choice of Organ
Experience has shown the risk factors for breast cancer to be heredity, late
first pregnancy, failure to breast-feed or stopping too soon, oversized breasts
and alcohol consumption. Our biographical research has also shown that
chronic or acute mental disturbance of the I-You relationship can be a factor
in disposing a patient for breast cancer. Prior to puberty such disturbances
relate mainly to breaks in close relationships, after puberty to profound
disappointments in physical and psychological heterosexual relationships.
This is not surprising when you consider the breast as the organ of a mother's
natural loving devotion in body and soul to the child which is still entirely
within her sphere. Later, this experience, still entirely unconscious in the
small child, can be transformed into a healthy I-You relationship if the
processes of metamorphosis are not disturbed.
Our patient gave birth late and breast-fed for only a few weeks as she
wanted to return to work as soon as possible. The early death of her beloved
father, the loveless relationship with her mother, the failure of her first deep
friendship, the sudden end of a deeply fulfilling relationship in middle life,
and the tensions with her husband, which lasted until her death, were all
acute and chronic hurts in this sphere. They followed an almost regular 7-
year rhythm, starting with her 9th year and continuing until the appearance
of the tumor and finally her death. It therefore appears that symptoms in
both body and soul might be responsible for the choice of organ.
Treatment
Anthroposophically-extended treatment is directed on the one hand towards
the illness itself and on the other towards the levels of life, soul and spirit
(ego), and thus the patient's general condition.
Medical Treatment
From May 1984, immediately after her operation when she was 58, the
patient was given virtually uninterrupted mistletoe therapy with Abnoba
viscum. The following medication relevant to the tumor was also given:
Tamoxifen V/84-VI/85 (discontinued owing to progression)
Orimeten (aminoglutethimide) VI/85-V/86 (discontinued owing to progression)
FEC-Chemo, twice IV/89 (discontinued owing to progression)
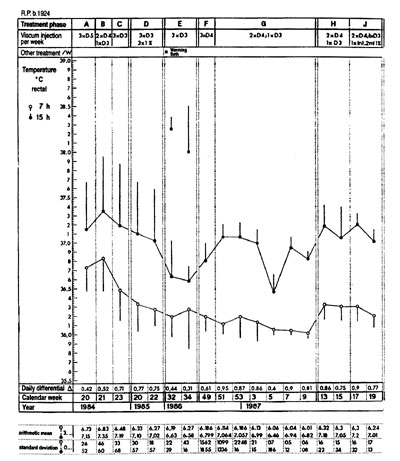
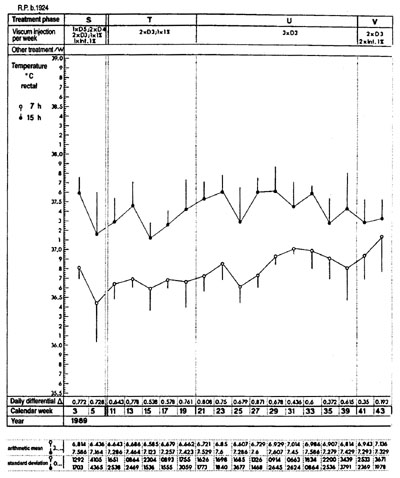
The patient's temperature was not taken prior to commencement of
treatment. At commencement of treatment the daily differential was low,
0.42 degrees C. It improved rapidly to > 0.7 degrees C during the early weeks. The
temperature chart thus confirms the observation that mistletoe therapy improves the chronobiologically relevant diurnal temperature range, establishing rhythm.
The reduction in amplitude in calendar weeks 32-35/85 correlates with
the patient having twice weekly hyperthermic baths during this period.
Maximum body temperature while in the bath is shown above the curve.
Afternoon temperatures on bath days were not included in the evaluation. In
the period immediately following this, the range rapidly increased to > 0.7
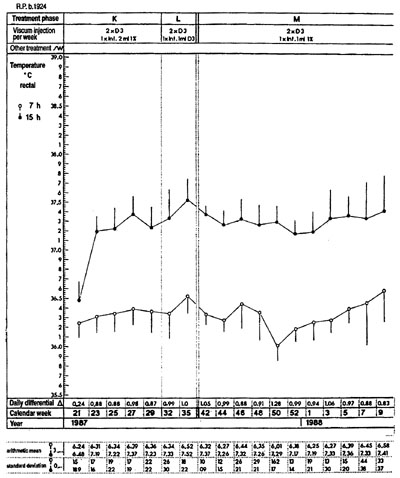
degrees C, despite changes in dosage, m treatment stages I, K, L, M, S and X, Abnoba viscum infusions were given once a week, in phase V twice a week. The
temperature did not change on infusion days nor did the averages or
standard deviations. The worsening of the daily differential in weeks 5/87
and 21/87 was due to intercurrent infections.
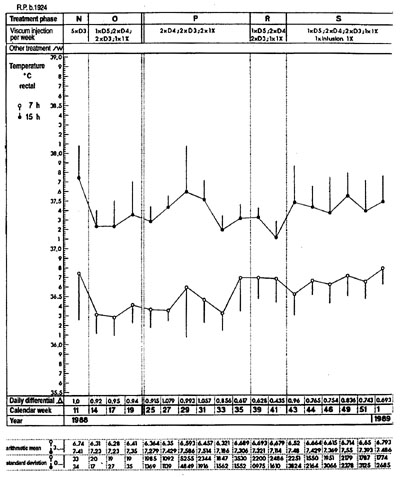
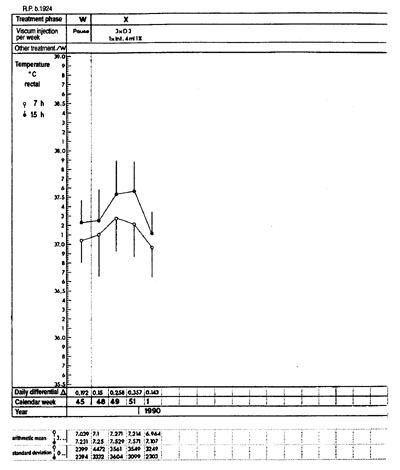
From calendar week 31/89 the diurnal temperature differential
worsened noticeably and did not return to normal despite varying doses of
Viscum and a 14-day interruption of the injections. This coincided with the
appearance of the liver metastases, which became manifest 3 months after the
appearance of the liver metastases, which became manifest 3 months after the
attempt to reopen a bronchostenosis with extensive atelectasis. Temperature
measurement was discontinued 10 weeks before the patient died. The
various changes in Abnoba¨ viscum dosage mirror efforts to halt the gradual
progression. It also shows the physicians' uncertainty owing to the lack of
sure criteria on which to base assessment of Viscum dosage. The following
criteria were used to determine dosages for this patient:
- The patient's statement as to how she was feeling, the temperature chart
and the Merieux score. The question as to the significance of eosinophils
for the progress of the disease had not been asked at the time. Subsequent
consultation of the notes shows > 360/mcl, determined in calendar week
20/85 and during infusion treatment in calendar week 3/89 as well as for a
time after chemotherapy.
- The Merieux Multitest was carried out from calendar weeks 22/85 to 3/89.
The score ranged from hyperergic at the beginning to normergic later on. It
therefore showed no correlation to the various dosages nor to the patient's
taken by the disease.
Retrospectively it becomes obvious that the patient's progress was
exceptional, given that the life expectancy had been up to one year, based on
statistical averages in 1984. Her condition was relatively good for the first 4
years. From 1988, this deteriorated owing to dyspnea on exertion and atelec-
tasis. For the final 3 months she was almost entirely bedridden. She herself
was convinced that the mistletoe therapy had given her very considerable
was convinced that the mistletoe therapy had given her very considerable
help. In retrospect, it has to be admitted that the question of optimum dosage
cannot be answered on the basis of the available data.
Eurythmy Therapy
The patient first had eurythmy therapy, both individually and in a group,
during a 3-week stay in hospital in May 1984. Movement diagnosis showed
the following:
The chart shows the following data, from the top: 1) Treatment phases showing
Abnoba viscum dosages. 2) 14-day mean values and standard deviations of morning
and evening temperature. 3) Diurnal differential 4) Calendar week and year. 5.
Merieux Multitest score (+ - - - +). 6. Absolute lymphocyte, monocyte and
eosinophil counts.
1 Contraction and expansion
Her first movement was jerky, striking the breastbone with her fists. She
remained in this position, and the gesture was more one of collapsing
inwards than of making a controlled movement. It took her a week to gain
sufficient strength to make the polar gestures of contraction and expansion
smoothly.
2 Threefold walking
The patient had her own way of achieving a flowing transition between
lifting, carrying and placing. She kept her eyes on the ground and the lifting
gesture of the foot had the "character" of N. (Exaggerated lift of the heel
towards the buttocks.) With the big toe stretched upwards during the
carrying phase, the foot went into the third, "placing" phase. During all 3
phases the pelvis was thrust forward and the chest region drawn back.
Carrying and placing soon came under control when practiced, but she had
difficulty with lifting for over a year.
3 I A O
The I gesture (bringing uprightness to the whole body) was done from the
feet upwards to the level of the stomach. Only one leg formed the A angle,
which meant a shift from the vertical position of I. The patient entirely failed
to notice the rounded 0 to be made by the arms. Having watched the whole
sequence for a second time, I and A were done in the same way over again.
To do the 0 she opened her arms and then angled them, bringing her fingers,
bent over, to rest on her chest. Initially the patient was unable to remember or
imitate the sequence in which she had performed the gestures. An alert "I
look into the world" was not possible. The flow of movement was hesitant
and searching and went too abruptly into the final stage. There was no sign of
feeling impulses. The whole middle sphere appeared to be hollow and rigid.
After a considerable time and much effort the patient succeeded in doing
the IAO exercise very harmoniously. She then drew strength from it and
used to say: "My IAO has helped me."
The aim of the therapy was to achieve the sequence O E M L E I B D,
which Rudolf Steiner had indicated for a patient with breast cancer:
Initially, the patient practiced out of a sense of duty. The L gesture was
made without any awareness of the movement. After we had alternated
practicing it with the arms and experiencing it inwardly as a movement
picture, the patient managed to put some life into the sound. After observing
the laws of the L in circulating water and plant growth, she said: "The L is
teaching me to understand and love nature in a new way."
Next, the patient had to take hold of 0 and E. We began with the large 0
and E exercise. The patient noticed that she became increasingly good at
remembering the movements;parallel with this went an increase in
self-confidence. When praised she smiled and breathed deeply. Alternating 0
(reaching outwards and embracing lovingly) and E (finding oneself and
standing firm) had the effect of quickening the patient inwardly and giving
her a sense of being protected. "It stops me from getting deeply sad."
The patient continued as an outpatient from September 1985 to April
1986. It was noted that once she had left the hospital the vowels immediately
lost their inner force, becoming no more than posturings on some occasions.
With practice at home more flow was gradually brought back into them.
"Feeling" and "character" of the sound showed clearly that the patient was
succeeding in taking hold of space and bringing the flow of movement into
the muscle tone and thus into quietness. Although her 0 gestures were timid
in "movement" and "character" and almost non-existent in "feeling", many
protective B layers were formed around the 0, so that the "feeling" content of
the vowel entered into a proper relationship with "movement" and
"character."
The leg exercises for both vowels and consonants had to be done mostly
while seated. Consonant jumps were not possible. The lung metastases
caused dyspnea. The patient's chest, initially feeling almost like a suit of
armor, became more mobile and permeable as a result of forming the M
gesture, which was done in all three directions of space. M performed with
the feet while seated was most effective at bringing about relief in proper
breathing.
Family commitments and a holiday meant a 4-month break in eurythmy
therapy. In August and September 1986 she had to be readmitted as an
inpatient. Potential for movement was limited, with contractive tendencies
uppermost. The movement diagnosis was much the same as in 1985. Inner
restlessness, a freezing posture and hasty movements were paramount.
Several pauses were necessary between exercises in order to practice letting
go and to activate exhalation. Treatment began with rhythmical exercises
with the ball and foot roller. After this the patient's breathing was deeper and
quieter. She slept better at night and did not wake at 2 a.m. as often as before.
She was taking part in group and individual therapy. We noted that this time
she observed her fellow patients and at the end of her stay also asked
questions about further therapy.
She now became an outpatient for just under 2-1/2 years. Her domestic
situation became increasingly difficult. She had been accustomed to success
in her professional life, where her orders had been carried out. Now her only
tasks lay within the family circle where she wanted to create order. But she
always met with resistance and rejection. This made her put up barriers
between herself and all those around her. By contrast, her own inner world,
though small and delicate, had now come alive: "My 0 and E give me the
strength to breathe. My D now overcomes my constipation." When the
protective B layer was particularly feeble she was shown P. She made the
gesture spontaneously many times, began to laugh and said: "That makes me
feel so well, like on the beach on Rhodes." She made a wide P gesture,
bringing it in from the space around her and up close to her body. I then
asked her to follow me in doing T. She lifted her arms as though to make a
large gesture, but it became as though held back by the chest region and
ended small, with a very hard knock on the top of her head. She listened
within herself to what had happened and then stretched upwards in the I
gesture. She made this with her whole body!
We frequently brought the sequence O E M L E I B D to life, cultivating
the individual sounds or groups of them, and the polarities. The patient had
great difficulty doing the exercises with her legs, as her ego had trouble
taking hold of the lower limbs. She practiced alone for a considerable time.
When she returned to the therapy sessions she had become much older
inwardly, despite the care taken with her outer appearance. She was weaker
both mentally and physically and could only do the exercises with the help of
the therapist.
The main problem was dyspnea. Propped up on her lower arms she
fought for breath. For a considerable time only major and minor chords
reached her, and she was able to expand and contract her fingers to the
music. The regular swing between chords turned into the iambic rhythm:
minor-major, minor-major. We ended the exercise when she managed a long,
deep breath. Then she looked at the instrument and lovingly stroked the
strings. I offered to let her take the small lyre home with her. She hesitated,
but then said in a hard voice: "Something so beautiful can only happen here."
The patient was unable to come for treatment for some time but returned
after I rang her. Her first words were: "My L protects me from all sides, like a
sphere." She never spoke about the difficulties she had at home, but the effect
of the constant attacks on her showed in the whole way she behaved.
In February 1989, the patient spent 20 days in the hospital. We had to
make long pauses between exercises. Once again the main problem was
dyspnea. We practiced the asthma sequence very slowly. Her great
enthusiasm for the eurythmy sound gestures burned brightly once more.
Previously we had succeeded in warming her cold limbs with eurythmy, but
now we only managed to warm her arms for short periods, while her feet
remained cold. On the day she left I witnessed her meeting with her husband.
His spiteful remarks brought everything we had achieved with such
difficulty crashing to the ground.
Her admissions to hospital became more frequent. In July 1989, she no
longer had the strength to do the exercises herself. Her eyes shone when the
gestures were made for her. At Christmas 1989, her family let her put up a
print of the Sistine Madonna in her cold home. She reported briefly that a
suffocating attack had resulted in an emergency admission to the local
hospital. While there she had constantly thought of the I gesture, and now
she was being helped by the I gesture of the Sistine Madonna.
Conclusion
The patient's withdrawal from the world and her anxiety brought about
strongly contracting movements. She was caught up inside herself and
scarcely able to notice what was going on around her. The therapy gradually
helped her reestablish some connection with those around her. Self-confidence
and self-assurance grew as she became better at performing the
exercises. Her movements, small and stiff at first, began to breathe. Tensions
at home in the intervals between therapy sessions always brought set-backs.
As life drew to a close her gestures for the speech sounds were light and
wide. She had already extricated herself somewhat from her body. Throughout
the treatment the patient had always made great efforts to create a balance of "movement", "feeling" and "character" for the separate sounds.
Mental Exercises as Therapy
Inner or mental exercises are an effective therapeutic tool. The life organization
can be strengthened and brought into a new relationship with both
body and soul. An exercise in observation that strengthens purposeful acceptance
of the world through the senses can help turn a person's attention
outwards. As a polarity to this, an exercise in writing with the left hand helps
to bring the will into a person's actions. The patient did these exercises
faithfully for a long period though later on they had to be modified.
Therapeutic Talks
Inherent in the talks about her biography was the concept that both internal
and external destiny has its roots in prenatal events. This can lead away from
blaming others and help the patient begin to look for the meaning of her own
life and illness. Towards the end she acknowledged the wish to find a new
relationship with her mother, who had meanwhile died, and to discover
what she could do to change her relationship with her husband and
daughter. She made an effort to bring rhythm into her daily routine and to
cultivate the cultural interests she had neglected for so long.
Summary
The patient was treated by us for 6 years. After surgical treatment of her
advanced cancer, her statistical life expectancy was approximately 1 year.
Two years after the operation she was so much stronger that she felt better
than she had for many years. She made every effort to overcome sensitivities
within the family and to smooth over the divisions that had arisen. She
succeeded in small ways. During the 6 years following discovery of the
disease the lung metastases grew slowly. A year before she died she suffered
an acute bronchostenosis that required emergency hospitalization. As she
fought against dying of suffocation her husband bent over her and asked her
to forgive him. Later she spoke of this as the high moment of her life, but to
her immense sadness the open door was closed once more. Five months
before her death she began to experience pain in the upper abdomen as a
result of massive liver metastases. She was dignified and fully aware
throughout the final days of her life.
We have shown how the development of functional carcinosis, i.e. a
disposition to cancer, can be deduced from the biography of a breast cancer
patient, m the first half of life various events and the way they were dealt
with led to a retarding tendency that brought delay in transforming the
forces of youth during the various developmental stages. In the latter half of
life premature aging tendencies showed that bodily development had now
accelerated. The ego organization was not able to suppress the tendency of
cells to proliferate in an organic region that had become particularly
susceptible as a result of the quality of the experiences described and the
inability to overcome them. The overall effect of medical treatment,
eurythmy therapy, mental exercises, and growing awareness of her
particular life's problems meant that the patient experienced a length and
quality of life far in excess of the original prognosis.
Hans Werner, M.D
Hans Broder van Laue, M.D.
Elke E. van Laue, curative eurythmist
Klinik Oeschelbronn
D-75223
Niefem-Oeschelbronn
Germany