Pilot Study on Steiner's Medical History
Questions in Relation to Clinical Syndromes
(Original title: Pilotstudie
ueber die Anamnesefragen R. Steiners und ihre Beziehung zu
klinischen Bildem (II. Teil) Merkurstab 1995; 48:161-176. English by
Christian von Amim, FIL. (originally part 2 of a series))
Manfred Weckenmann, M. Kitschmann,
E. Rauch, K. Trageser, G. Moellenbruck and
M. Wormsbecher
Vol. 12, Nr. 4
In this article we intend to report on the methodology of recording key
symptoms in accordance with Rudolf Steiner's medical history questions and
their relationship to one another.
1 Methodology
1.1 Nomenclature
The totality of recorded patients is called the total group. Principal subdivisions
(e.g. sex, age) are called subgroups, subdivisions according to constitutional and functional perspectives (e.g. autonomic functions) classes and
significant symptoms characteristics, insofar as they do not refer to the
medical history questions. Rudolf Steiner's medical history questions are
called key questions, the answers key symptoms. Excessively strong/weak
affinity between 'I’ and astral body on one hand and etheric and physical
body on the other is described as Excessively strong/weak intervention. A group
of key symptoms which leads to similar conclusions about the action of the
human constituent elements is described as concordant, one which leads to
contradictory conclusions discordant.
Apart from the occurrence of key symptoms that go in the same direction,
account is also taken, on occasion, of the exclusion of a key symptom
that is the opposite. Characteristics referring to opposite key symptoms of
equal weight are called ambivalent.
Words in single quotes are used in analogy or as key words, e.g. 'salty'
for salt requirement. This is a concession to the brief nature of the text. Words
in double quotes are quotations, although they may not always be grammatically
true to the original.
1.2 Patients
Characteristics and key symptoms of 166 patients from the Department of
Internal Medicine of the Carl Unger Clinic in the years 1966-1967 were
analyzed. Case notes with serious gaps were excluded.
1.3 Data recording
A medical history questionnaire was completed by the patient, if necessary with
assistance from the physician. The answers were not to refer to the current
state of illness but to the time before the illness. The questions were thought
to be unambiguous and were answered freely. The physician filled in a
diagnostic questionnaire. Rhythmological data were recorded by an assistant.
1.3.1 Medical history questionnaire
According to Steiner 'dreaming,' 'disturbed sleep,' 'lethargy,' 'short sightedness'
and the need for sweet things indicate excessively weak intervention,
the opposite symptoms and vertigo during external mechanical processes
excessively strong intervention.(7,8)
In order to get unambiguous answers to Steiner's key questions,(7,8) the
following questions were asked:
- To assess dreaming: Do you dream a lot during the night? What is the
nature of your dreams?
- To assess sleep: Do you often take hypnotics? Which? Do you have
difficulty falling asleep? Do you wake frequently? Approximately how
often?
- The question concerning mobility, activeness or lethargy had to be adapted
to the patients: Is it an effort to do anything? Yes? No? Since when?
- In the question concerning sight, confusion with presbyopia had to be
excluded: Are you nearsighted? Farsighted? Since when? Do you have to
wear glasses all the time? While reading?
- A question was asked about the "longing" for salty or sweet foods: Do you
generally like strongly salted foods? Sweet foods? Sour foods? Bitter foods?
We specifically asked about highly salted food since medium salting tends
to be the rule. It was stated that the question applied only to the desire, not
to the way the patient acted on rational grounds.
- The question about vertigo caused by external mechanical processes, e.g.
by rapid rotation of the body, was specifically differentiated: Do you easily
become dizzy? When dancing? When turning suddenly? When bending
over? When straightening up? When getting up in the morning? When
looking down? (It was not asked whether the sensation of vertigo was
revolving, or swaying etc.).
(The question about slow or fast growth had been wrongly put and could
not be included in the analysis. This does not matter in so far as it refers more
to the etheric body.)
The question about problems with eliminations was dealt with separately
as Steiner only says in general terms that they allow conclusions to be
drawn about disorders in the cohesion of ‘I’ and astral body on one hand and
the etheric and physical body on the other. But he does not specify how. The
questions asked were:
- Do you have a daily bowel movement? How often? Do you regularly use
laxatives? Yes? No? Occasionally? Which? What, in general, is the
consistency of your stools? Firm? Soft? Thin? Traces of blood? Traces of
mucus?
- Do you perspire easily? Where on the body?
We did not find a satisfactory formulation for assessing the passing of
urine. The question about menstruation was deliberately excluded since it is
to be examined in a special group.
1.3.2 Diagnostic questionnaire
Sex, age and body mass were determined for the formation of subgroups.
Autonomic functions were assessed on the basis of pulse rate, respiration
rate and the pulse-respiratory quotient.(2) The following questions were also
asked: Do you feel cold easily? Do you often have cold hands? Cold feet?
(These questions also cover the symptom of cold, clammy extremities). And:
Do you feel best in the morning, at midday or at night?
The following was asked for the classification relating to development
during childhood and youth < 21: Were you a strong or not very strong child?
What was your energy state from age 6 to 13? From age 13 to 20? Did you
have a nice childhood? Did you enjoy your youth? Did you suffer any
shocks? At what age? Did you have periods of sustained worry or distress?
The following was asked for the classification relating to basic mood: Do
you tend to get depressed? The physician also made an assessment whether
the patient was in principle depressed and despairing - agitated, restless,
fidgety - calm, indifferent.
For the classification relating to complexion the physician noted: skin color
- hair color - color of eyes. Mixed complexions were decided specifically
according to skin and hair color.
Constitutions were classified as leptosome, athletic and pyknic Kretschmer
types, as well as a mixed types.(3)
1.4 Methods of examination
Body mass was calculated according to Broca:
Body weight (kg) x 100 / (height (cm) -100).
Overweight people thus have a body mass index >100%, underweight
people <100%.
Pulse rate, respiration rate and pulse-respiration quotient were deter-
mined on all patients during the working week after 9 a.m. while resting in
bed, always by the same assistant. Individual measurements were repeated
at approximately the same time. Pulse and respiration rates were counted for
3x1 minutes each, with the pulse-respiration quotient based on the arithmetic
mean. The pulse rate was taken at the radial artery by palpation. Patients with
weak heart contractions were excluded. The respiratory rate was
determined visually and unnoticed by the patient.(6) For further methodology
see reference.(9)
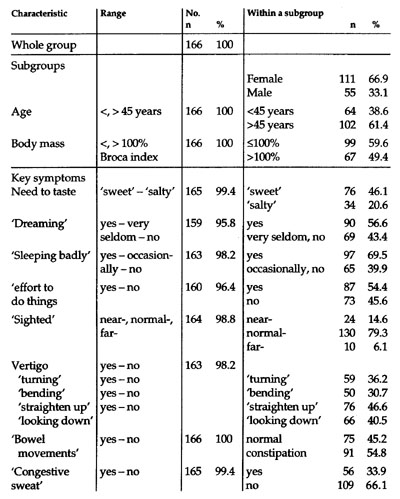
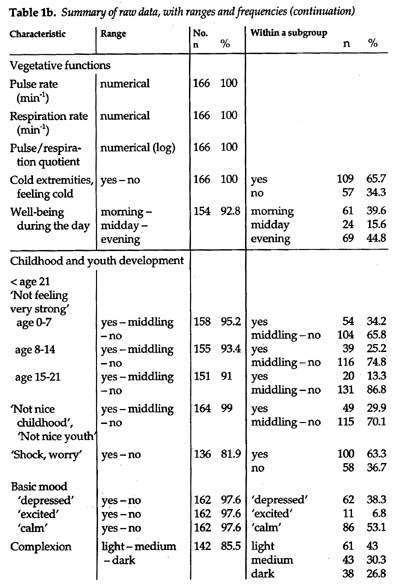
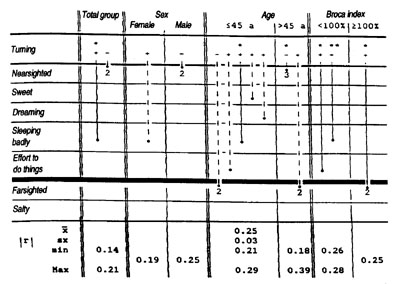
Table 1a. Summary of raw data, with ranges and frequencies.
Constitutions according to Kretschmer types(3) were established visually by a
trained physician.
1.5 Analysis of raw data
Table 1a shows the characteristics and their rating, derived from the raw
data, e.g. Yes - No or numerical. Characteristics were encoded, e.g. Yes: 0,
No: 2, neither nor, undecided and equalizing values: 1. Individual means for
pulse rate, respiration rate and the pulse respiration quotient during the patient's
inpatient period had been previously determined by Trageser.(9)
Further calculation of the pulse-respiration quotient was done logarythmically, distribution being abnormal.(2)
1.6 Statistics
Normal distribution was characterized by mean value and standard deviation,
differences between the latter were estimated by t-test and, for non-normal
distributions, by Wilcoxon. Frequency distributions were evaluated using
the chi-squared test, partly against one another, partly against expectation.(1,4)
Comparisons between two scores were done by Pearson correlation coefficient
after controls with the chi-squared test brought identical results, p <0.001
is judged to be highly significant (h.sig.), p <0.01 as very significant (v. sig.), p
<0.05 as significant (sig.) and p<0.1 as statistically conspicuous (st. con.).
No alpha adjustments were made. Always demanded by statisticians,
they hardly ever appear in medical publications. The method is meaningless
for our purposes because there is no random sample survey in a statistical
sense, and the statement of probability is only intended to assist relative
assessment to form a personal judgment (personal information from
Burckhardt).
1.7 Presentation
The relationship between characteristics was intentionally not presented in
the usual form of contingency tables because in the 3 methods of calculating
short and long sightedness (see 3.2) there is no general reversibility which can
be expressed by + or - alone. Furthermore, the aim was to keep the grouping
of characteristics in the 2 classes of strong and weak intervention optically
apart. Finally, the data was intended to be presented in a more space-saving
way than with contingency tables. We therefore decided in favor of bar charts.
All results were printed at an angle so that they can also be read
diagonally.
1.8 Equipment
Equipment: Victor V 286, Statgraphics software ISBN 0-926683-06-3 (USA)
and Microsoft WORD 5.0.
2 Results
The characteristics are presented within overall and subgroups and in their
relationship to one another. For further data see tables la,b respectively.
2.1 The characteristics of the subgroups
In accordance with the usual distribution of admissions to a department of
internal medicine, approximately twice as many women as men were represented
(Table la). Age was x = 51.1 + 15.7 years (20-81 years). This was subdivided
into <45 and >45 because there were twin peaks in age distribution
(Table 1), because the menopause was to be included in the higher age group
and because earlier investigations had shown that Scleron was recommended by
Steiner as a geriatric medicine from age 40,(10) i.e. the aging process
becomes more pronounced after this. Approximately two thirds of patients
were >45 (Table la). Distribution according to sex was the same in both age
groups. Patients <45 are described as 'younger' and patients >45 as 'older.'
Average weight was x = 65.6 + 15.2 (35.0-140.3) kg with an average
height of x = 166.7 + 8.2 (147 -189) cm. 59.6% of patients had a body mass index
<100%, 40.4% >100% (Table la). Body mass also established the link to
Kretschmer types,3 with a Broca index of 84.4 +11.6% for the leptosome type,
99.0 + 16.3% for the athletic type, and 120.6 + 18.1% for the pyknic type.
Constitutions also correlated positively with the Broca index (r = + 0.74 p
<0.0001) but not with height and weight. Patients with Broca index <100% are
described as 'slim' and the others as 'corpulent'.
Fig. 1. Histogram of age distribution in the total group (n = 166 patients).
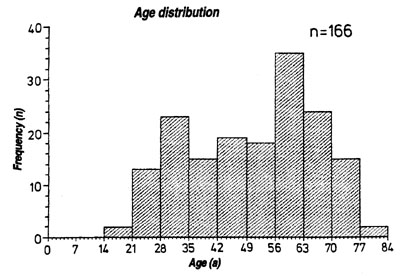
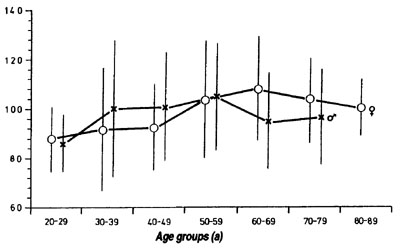
Fig. 2. Changes in body mass at different ages. Ill women and 55 men. Brackets
indicate standard deviation.
Correlations between the 3 subgroups showed a link between age and
corpulence only (r = +0.22, p <0.01). The 'younger' group was slimmer,
independent of gender, than the 'older' group (Broca index 92.4% vs.102.9, p
<0.01). But that relationship was not constant (Fig. 2). At an advanced age
corpulence went down again, from approximately age 65 in women and 55 in
men (which corresponds roughly to the different ages of mortality).
2.2 Key symptoms
2.2.1 Key symptoms in the total group (Table la, b)
- 'sweet,' 'salty': One third of patients had ambivalent taste requirements. Of
the rest, approximately twice as many preferred 'sweet' to 'salty'. Only
positive statements were included, so that 'not sweet' is equivalent to
'salty' and vice versa.
- night-time 'dreaming': Approximately half of all the patients dreamt
frequently. They were evaluated against the rest.
- 'sleeping badly': Approximately 70% of patients complained about dis-
turbed sleep ranging from slightly to seriously disturbed. 30% slept well.
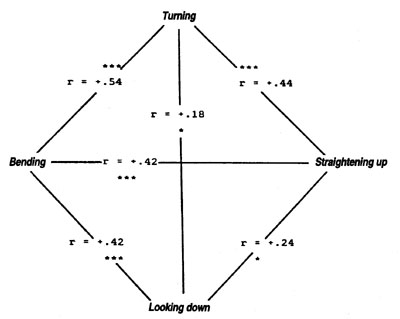
Fig. 3. The correlative relations between the 4 types of vertigo in the total group (n =
166). For symbols see legend Table 2.
- 'effort': Approximately half the patients complained about 'it being an
effort to do something'. They were evaluated against the rest.
- 'nearsighted', 'farsighted': Only 20.7% of patients were near or farsighted. Of
these, approximately two thirds were nearsighted and one third was
farsighted.
There was no age differential, which argues against the confusion of
presbyopia and hyperopia. The small number of cases of impaired sight
induced us to use 3 types of analysis:
1. nearsighted vs. normal sighted and farsighted as well as farsighted vs.
normal sighted and nearsighted;
2. nearsighted vs. normal sighted as well as farsighted vs. normal
sighted;
3. nearsighted vs. farsighted.
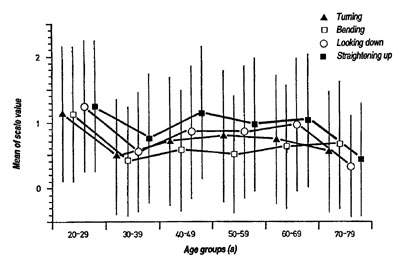
Fig. 4. The 4 types of vertigo by age in the total group.
- 'vertigo': 71.8% of patients complained about vertigo, mostly while getting
up (Table la). Since Steiner emphasizes vertigo caused by external
"mechanical processes," e.g. "by rapidly turning around,"(7) it was not clear
whether this also included bending down and straightening up again.
Neither the - roughly equal - correlation between the different types of
vertigo (Fig. 3) nor their relationship to age (Fig. 4) provided any help in
reaching a decision. As is shown by tables 2 and 3, 'turning' only
correlated in 35.7% of cases with key symptoms which indicate strong
intervention. In the remaining cases vertigo in the total/subgroups was
always concordant (31x) with characteristics of weak intervention. Since
'turning' could be typical - neurogenic vertigo connected with old age - its
occurrence in >70-year-olds was examined. Although there was no
frequency difference in comparison to the <70-year-olds (Fig. 4), there was
a slightly higher correlation with far-sightedness (r = + 0.35) in >70-year-
olds than in <70-year-olds (r = + 0.18 p <0.1). Thus vertigo from 'turning'
in 70-year-olds could be connected with excessive intervention. Therefore
the four types of vertigo were hypothetically linked with inadequate
intervention in the first instance, and only 'turning aged >70' was linked
with excessive intervention.
2.2.2 Key symptoms in the subgroups sex, age and body mass
The greatest differences were found between the sexes. There was a tendency
for women to 'dream' more frequently than men (61.9 vs. 46.3% p <0.1), to
'sleep more badly more frequently' (61.1 vs. 48.2% p <0.01), to have to 'make
a greater effort to start work' more frequently (61.5 vs. 39.2% p <0.05), to
complain more about vertigo when 'turning around' (44.4% vs. 20.0% p
<0.01), 'straightening up' (55.6% vs. 29.1% p <0.01), 'bending down' (38.9%
vs. 30.7% p <0.01) and 'looking down' (43.5% vs. 34.5% n.s.).
The age differential was low. 58.6% of 'older people' slept badly, but
'younger' ones still did so in 45.4 % of cases (p <0.1). With body mass the
surprising thing was that corpulent people rarely had to make 'more of an
effort to to do anything' than slim people (62.1% vs. 51.1% p <0.1) and slept
hardly any worse (60.6% vs. 49.5% p <0.1).
Thus women had a stronger tendency towards weak, men towards strong
intervention. Age and body mass did not demonstrate any certain relation.
2.2.3 Relations between key symptoms (Table 3)
Pairs of relations were treated as reversible, e.g. 'dreaming' - 'sleeping badly
vs. 'no dreams' - 'sleeping well.' In the tables, only one of the 2 pairs is linked
with a bar for reasons of clarity, e.g. 'dreaming' - 'sleeping badly' but not 'no
dreams' - sleeping well'. Only positive correlations are mentioned, e.g. positive correlation between 'dreaming' and 'sleeping badly,' and not the negative
correlations between 'dreaming' and 'sleeping well'. Such reversibility
applies only in a limited way to sightedness according to methods 1 and 2
(see 3.2.1)
In the total/subgroups there were altogether 39 sig.- h.sig. and 17 st.con.
concordances and only 2 sig. and 3 st.con. discordances with I r I = 0.14 - 0.4.
The correlations referred in descending order of frequency to: 'sleeping
badly' (28), 'straightening up' (18), 'dreaming' (16x), 'turning around' (14),
'effort to do anything' (12), 'bending down' (9), 'long and near-sighted' (3
each), 'looking down' (4), 'sweet' (2), 'turning aged > 70' (1).
While all types of vertigo except 'turning' correlated without exception
with the characteristics of a lack of intervention (see above) and 'turning' also
related 9 times to a lack of intervention, it also related 5 times to strong
intervention, although only in relation to sight.
This result came as such a surprise, that we wanted to test it by means of
a second method.
Every key answer was given a value such that 2 stood for an answer
indicating weak intervention, 0 for strong intervention and 1 for a mean,
indifferent value. Vertigo was no longer differentiated.
Fig. 5 shows the frequency distribution of the evaluation of the
individual key symptoms. Only sight clearly shows frequent indifference.
Fig. 5. Frequency distribution of the values 0,1 and 2 for every key symptom in the
total group.

0 stands for strong intervention, 2 for weak intervention and I/or indifference.
Every patient was then given a personal value by adding his of her
values together. A total of 0 clearly indicates strong intervention, a total of 12
weak intervention.
Fig. 6 shows the histogram of all individual evaluations. Distribution is
not normal (p <0.0001).
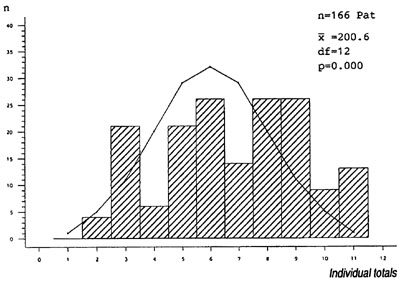
Fig. 6. Frequency distribution of the individual totals of assessments 0,1 and 2 (see
Fig. 5) of the 6 key questions compared to anticipated distribution in the total group.
To test this unexpected distribution, the theoretically possible
combinations of all three answers to the 6 questions had to be calculated: (a +
b + c)n, where a, b and c represent the three values 0, 1 and 2 and n the number of questions, here 6. In order to calculate the frequency of the
individual totals, the binomial formulation (a + b)1n was extended by (a + x)n,
with x = b + c, and the anticipated distribution calculated on that basis. (Here
we would like to express our thanks to B. Moellenbruck, who assisted us in
finding the solution to the mathematical problem.) Since the total of this
anticipated distribution did not correspond to the number of our patients (n
= 166), we reduced the anticipated values as a percentage so that their sum
also came to 166. Only then could comparison of class membership be made,
using the chi-squared method.
Fig. 6 shows that the flanks of the anticipated distribution have a higher
level of occupation than the center, particularly with reference to the high
individual totals. The difference is significant, with chi2 = 200.6 df 12 p =
0.000.
This result confirms that of the first method: the answers to the key
questions are not mixed arbitrarily but show an above average chance
arrangement in line with either strong or weak intervention. 36.8% of the
patients are, however, in the middle group with values 5-7.
This was followed by the question whether the gender difference
observed above could also be confirmed by this method. Fig. 7 shows the tendency among women for higher sum totals and among men for lower
ones (chi/n = 23.5 df 9 p <0.005).
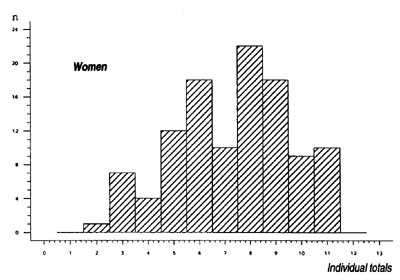
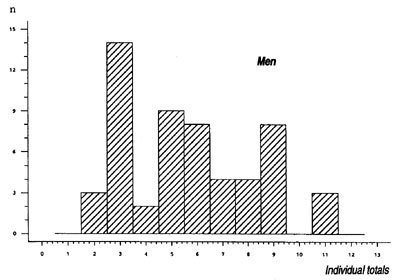
Fig. 7. Frequency distribution of individual totals (see Fig. 6) classified ace. h
(female above, male below). The two distributions vary (p < 0.005).
No differences were noted in the age and mass subgroups, which is in
line with the results of the initial method.
Thus we can see an above average chance arrangement of the key symptoms in
relations to either strong or weak intervention. This convincingly validates Steiner's
statement. Women overwhelmingly show a pattern of answers which indicates weak
intervention whereas men show one which indicates strong intervention. The result
is independent of age and body mass.
2.2.4 Discussion
The way in which the questions were formulated could probably be
improved, but even at this stage polarization was good with uncertain
answers relatively rare (Fig. 5). A greater number of the latter inevitably
occurred with sight, but there were nevertheless 41 usable correlations for
near- and farsightedness. In 31.7% of cases they were confirmed by various
calculating methods (see 3.2.1) or at least did not contradict one another. The
study should, however, be repeated with a larger number of near and
farsighted people.
Contradiction between the spiritual scientific and the empirical statement
about vertigo permits the following conclusions:
- If Steiner's statement is true, then 'bending down' and 'straightening up'
are certainly not vertigo caused by "mechanical processes." But in that
case the latter types of vertigo, including 'looking down', could represent a
new symptom, found by accident, of lack of intervention because of the
frequency of their relationship with other key symptoms. That is why they
were retained below.
- Differences between individuals might then disappear insofar as the
physician has not asked differentiated questions about the various types of
vertigo. But in two thirds of all patients with 'turning', discordance would
still have arisen between individuals according to Steiner, because in their
case 'turning' is overwhelmingly associated with symptoms of weak
intervention.
- If Steiner's statement is not valid, two thirds of discordances between
individuals caused by 'turning' would dissolve; they would remain with
one third.
The problem cannot be solved statistically, but that only became apparent
following empirical investigation.
Neither can the problem be solved by assuming a mistake in the notes of
the shorthand writer; this is unlikely in light of the text. The question
remains whether 'turning' is really an ambivalent symptom and Steiner, by
chance, only saw patients in whom it was associated with strong intervention and generalized on that basis.
Statistical assessment of the weight of individual key questions was
omitted because factor analysis is only of use if the answers to each single
question are distributed normally. This not being the case, as Fig. 5 shows,
only an estimate can be made in line with the frequency of the correlations
(see Table 3) and the low number of indeterminate answers (see Fig. 5). In
this light, questions about sleep, 'dreaming,' 'need for effort,' 'vertigo' are
very reliable. The questions about sight are meaningful but their value is
limited in practice because of the large number of normal-sighted patients.
The question about 'sweet' and 'salty' correlates less frequently than accords
with my practical experience. This may be explained by the fact that we
asked about the need to add a lot of salt to food (see 2.3.1). (See below about
constipation and sweating.)
The spectrum of correlatively significant key symptoms is very similar in
total and subgroups. Everywhere there is a strong relationship between 'dreaming,' 'sleeping badly,' 'need to make an effort,' 'turning' and 'straightening up.' Altogether this result accords well with experience from case
studies.
The degree of correlation is disappointingly low in the first instance (I r I
= 0.14-0.44) (see Table 3). This is due to the many detailed characteristics, as
is known from other studies, and would change immediately with the
creation of subgroups, which was deliberately omitted in order not to
overlook previously unknown subgroups, as will be confirmed later (see
parts in and IV). The low correlation coefficients, indeed even the individual
discordances do not therefore need to indicate unusability of the method but
may provide statistical room for maneuver to accommodate individual and
subgroup particularities which we still have to learn to read.
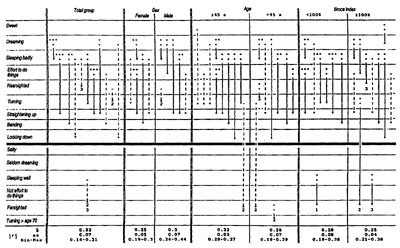
Table 3. Relations between key symptoms. Only
positive correlations, e.g. 'dreaming' - 'sleeping badly', are shown if
negative ones act as mirror image, e.g. 'dreaming' - 'sleeping well'.
Similarly only one pair of relations is named, e.g. 'dreaming -
'sleeping badly', when the other one, 'seldom dreaming - 'sleeping
well', is the inevitable consequence. Both pairs are entered when this
is not the case, e.g. with short and far-sightedness (see 3.2.1).
In the meantime our results have been tested by Kroez(5) using a sample of
108 women (56 with histories of or manifest breast cancer, 52 non-malignant
controls >40 years of age). The question was whether the relationship of the
human constituent elements was different in women who later developed
breast cancer than in women who have, as yet, no cancer. The women were
asked to say from memory how they would have answered Rudolf Steiner's
medical history questions between the ages of 21 to 30 and from approximately
40 to 45. To establish the relationship between the key symptoms the
results of both groups are presented here in summary.
The questions were:
1. Do you remember having dreams? Almost never, seldom, occasionally,
frequently, almost daily.
2. Did you have difficulty falling asleep or suffer from disturbed sleep?
Almost never, seldom, occasionally, several times per week, almost daily.
3. Do you tend towards far or nearsightedness (not presbyopia)? Farsighted,
nearsighted. The answer applies to both age groups.
4. Did you have a desire for sweet, salty, bitter or sour food? Yes, no.
5. Did you suffer from vertigo? Almost never, seldom, occasionally,
frequently.
6. How often did you have bowel movement? Approximately 1-2 times, 3-4
times per week, approximately once, 3-4 times, > 4 times per day.
7. Did you take laxatives? Frequently, occasionally, never.
Question 2 was formulated differently than in our case (see 2.3.1) in the
hope of achieving greater differentiation in the responses. This hope was not
realized.
In question 4 me expression 'highly salted' (see 2.3.1) was not included in
order to produce larger groups.
Question 5 was not differentiated (see 2.3.1), since differentiation offered
no advantage (see 2.3.1).
A score was produced from questions 6 and 7. Scoring took place
according to our results which will be published in part V: constipation is an
indication of lack of intervention.
This left 6 key answers. A score was calculated for every answer and
from this a total score for every woman. Correlation between the single
scores and the total score was then examined. Below, the results for age 21-30
always come first, followed by those for age 40-45.
- 'sleeping': ( r=+0.26 p= 0.0074; r=+0.0076 p= 0.938)
- 'dreaming' (r=+0.45 p= 0.0000; r=+0.41 p= 0.0000)
- 'sight' (r=+0.21 p= 0.0029; r=+0.29 p= 0.0033)
- 'taste' (r=+0.54 p= 0.0000; r=+0.44 p= 0.0000)
- 'vertigo' r=+0.25 p=0.01; r=+0.18 p=0.06
- 'constipation' (r=+0.58 p= 0.0000; r=+0.34 p= 0.0005)
This confirms our results in principle. That the correlations are partly
higher than in our case (see 3.2.3) is due methodologically to the way the
groups are formed. The reassessment of vertigo (see 3.2.1) is confirmed. The
new formulation of 'salty-sweet' resulted in more exact relations than in our
case (Table 3). The result for 'sight' is again remarkably good despite the
small groups.
The question about 'falling asleep and disturbed sleep' is less suitable in
this form. Our formulation (see 3.2.1) proved to be more accurate.
Thus it emerges that Rudolf Steiner's key questions, with reference to the
anthroposophical assessment of key symptoms, are very consistent within
themselves, provided that the 'vertigo' symptom is reassessed. This is all the
more remarkable as the content of the questions is very heterogeneous.
Given that the key symptoms allow conclusions to be drawn about the
highest constituent elements of the human being today, the 'harmlessness' of
the questions comes as something of a surprise. No psychoanalytical, psycho-
social or biographical questions! And yet they are the key to anthroposophical
treatment. In my opinion this can be explained in that the ‘I’ of the patient
does not need to be discernible to the physician but only the intensity of its
intervention.
Another factor, too, appears to be of significance: the more physicians
remain phenomenological, truly "shallow," in their observation, the more
they school themselves to investigate the depths by esoteric means and not
by speculative deduction and spiritist methods (see 1.3).
The questions about key symptoms have proved so useful in making
anthroposophical diagnoses that I would not want to do without them during consultations. Moreover they train the faculty of perceptual judgment.
Nevertheless, questions remain open, e.g.: what does it mean that some
questions focus on very constant characteristics ('sight') and others on
changeable ones ('sleep'), that some are more directed at the body ('taste')
and others more at the psyche ('dreaming')? This should be the starting point
for more in-depth studies.
Manfred Weckenmann, M.D; M. Kitschmann, M.D.,
E. Rauch, M.D., K. Trageser, M.D., G. Moellenbruck, M.D.
and M. Wormsbecher, M.D.
Filderklinik
Im Haberschlai 7
D-70794 Filderstadt
Germany
References
1 Haseloff OW, Hoffmann HJ. Kleines Lehrbuch der Statistic. Berlin: W. D. Gruyter und Co. 1965.
2 Hildebrandt G. Die rhythmische Funktionsordnung von Puls und Atmung. Z angew Baeder-und Klimaheilk 1969; 7:533.
3 Kretschmer E. Koerperbau und Charakter. Berlin: Springer 1977.
4 Pfanzagi J. Allgemeine Methodenlehre der Statistik II. Berlin: W. D. Gruyter 1974.
5 Kroez M. Ueber Angst, Vegetativum und konstitutionalle Aspekte bei Mammakarzinom-Patientmnen. Inaug. diss. publ. prepared 1995.
6 Reichel H, Weidlich F. 1st durch Zaehlen von Puls- und Atemfrequenz ohne apparativen Aufwand die Wirkung von Badekuren erkenntlich? Arch Phys Ther (Leipzig) 1959; 5:338.
7 Steiner R. Spiritual Science and Medicine (GA 312), lecture of 25 March 1920. Translator not known. London: Rudolf Steiner Press 1975.
8 Steiner R, Wegmann I. Fundamentals of Therapy (GA 17), chapter 19,4th case. Translated by E.
Frommer and J. Josephson. London: Rudolf Steiner Press 1983.
9 Trageser K. Untersuchungen zum periodischen Verlauf des Puls-Afem-Quotienten und der Koerpertemperatw bei intemistischen Klinikpatienten. Marburg/Lahn: Inaug. diss. 1986.
10 Weckenmann M. Das Arzneirnittelbild von Plumbum im Spiegel von Argentum II.
Merkurstab 1990; 43:108