Translation of an article in Beitrage zu einer Erweiterung der Heilkunst, Juli 1980, No. 4.
Translator: A. R. Meuss FIL MTG.
Origins of the CSF
The CSF is secreted into the ventricles of the brain from
the choroid plexuses. "Choroid" derives from "chorion", the
vascularized embryonic envelope; the vessels form the placenta.
The ventricles of the brain are invaginated at an early
stage by the choroid plexuses, fringe-like vascular processes exactly the same
in nature as the placental chorionic villi. The escape valves (granulations)
are also of the villous type (v. i.).
Like the embryo, the brain is floating in fluid. Brain and
embryo are thus protected from pressure and given the freedom to grow and
develop their intrinsic form. In both cases, the fluid is secreted by an
epithelium — the epithelium of the amnion in the case of amniotic fluid, and
the choroid plexuses in that of cerebrospinal fluid. The head with its brain
floating in CSF retains this embryonic feature as a basis for its involutional
tendencies. In the case of the brain, the fluid is secreted against an osmotic
pressure gradient; being in osmotic hypertension, the brain would otherwise
take up water. There is a tendency for the brain to swell, to become
oedematous, and this is counteracted by the secretion of the CSF which forms a
protective envelope around it.
The greater part of the CSF is produced in the two lateral
ventricles (I and II), and enters the third ventricle (III) on either side
through the interventricular foramen. The central part of the third ventricle
narrows to form the aqueduct, and the CSF passes through this to the fourth
ventricle (IV), leaving it by the lateral apertures (Fig. 1, 2 and 3).
The CSF does not just go anywhere after this, but is
collected in a kind of sac formed by the arachnoid. The arachnoid is
impermeable to water and the brain rests on it like on a water-filled cushion
(Fig. 1). It is therefore not floating in the usual sense of the word. The
space inside the cushion is known as the subarachnoid space. In the superior
median line of the brain, villus-like elevations protrude from this space into
the superior sagittal sinus. These are valves through which the CSF escapes
(arachnoid or pacchionian granulations). Being enclosed in a cushion, the CSF
becomes the receiver, distributor and conductor of the alternating pressures
transferred to the brain via the CSF from the respiration and pulse. More of
this later.
Fig. 1. The
circulation of the cerebrospinal fluid in the cavities within the brain.
Circulation of the CSF
The total volume of the CSF in the cranium and vertebral
canal is 135 ml. This is distributed as follows:
In the subarachnoid space (water-filled cushion)
100 ml
Of this, the cranium contains 25 ml
and the vertebral canal 75
ml
The ventricles of the brain contain
35 ml
500 ml of CSF are produced daily, so that the quantity of
135 ml is replaced almost four times in the course of 24 hours. This also
reveals the vital importance of the peripheral escape valves; without them, the
brain would be destroyed by water pressure within a short time.
The CSF contained in the cranium (25 ml + 35 ml) actually is
renewed approximately eight times in 24 hours. In the cranium, the source and
the outflow point (escape valves) lie closer to each other than in the
vertebral canal where renewal occurs at a slower rate. There, in the vertebral
canal, the fluid is like the water in a backwater, in a lagoon cut off from the
open sea and its wave movements (D. W. C. Northfield 1973).
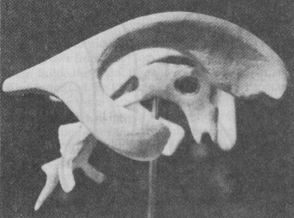 Fig. 2. Cast of the
cerebral ventricles (anterior aspect to the right). The curved form of one of
the lateral ventricles can be seen; between the two lateral ventricles lies the
third ventricle and this continues down into the cerebral aqueduct (narrow
tube) and then the fourth ventricle. The end of the narrow tube continues into
the central canal of the spinal cord. The hole in the third ventricle is in
life filled with a solid strand connecting the two hemispheres (commisure). To
the right above it, the place may be seen where the ventricles communicate
through the interventricular foramen.
Fig. 2. Cast of the
cerebral ventricles (anterior aspect to the right). The curved form of one of
the lateral ventricles can be seen; between the two lateral ventricles lies the
third ventricle and this continues down into the cerebral aqueduct (narrow
tube) and then the fourth ventricle. The end of the narrow tube continues into
the central canal of the spinal cord. The hole in the third ventricle is in
life filled with a solid strand connecting the two hemispheres (commisure). To
the right above it, the place may be seen where the ventricles communicate
through the interventricular foramen.
The CSF pressure can be measured inside the cranium, in the
ventricle, and in the lumbar region. In the lumbar canal, the pressure is equal
to that of the dense venous plexuses in that region:
150 cm column of
water = 11 mm Hg.
The pressure in the ventricles on the other hand is slightly
below zero when the subject is sitting down. If the pressure is determined below
the cerebellum, shortly before the CSF leaves the cerebellomedullary cistern,
it will be found to fluctuate between 40 mm and minus 85 mm CSF in a person
standing upright. At this point, beneath the cerebellum, the CSF therefore has
to be aspirated through the needle, as it will not escape under its own
pressure. "This means that during our waking hours, for about two thirds
of our life, the intracranial pressure is at zero or below" (D. W. C.
Northfield 1973). Negative pressures are easily thought of as suction forces,
and it is possible to think of suction forces involved in CSF production.
In the venous spaces (venous sinuses) into which the valves
or escape locks of the CSF project, the pressure is permanently below that of the CSF itself. These pressure
differences give rise to a "dynamic circulation of the CSF" which
takes place between the sites of secretion, i.e. the plexuses that are the
point of origin within the brain, and the CSF valves or sites of escape at the
surface of the brain. Arterial blood produces the fluid, venous blood receives
it. The brain and the spinal marrow are placed within this special fluid
circulation system. If this circulation ceases, or if it is obstructed by coagula
or pressure from a tumor at one of the narrower points, brain function is
immediately threatened.
Let us now consider the CSF circulation in comparison to the
blood circulation. Whilst the CSF is replaced four times a day, 1,200 ml of
blood pass through the brain in one
minute. This reveals the enormous difference between the slow movement of
the CSF on the one hand and the tremendous acceleration in the movement of the
blood on the other.
Fig. 3. Ventricular
cavities in the human brain (seen from above).
I-IV = 1st — 4th ventricle
a = interventricular
foramen
b = cerebral aqueduct
c = foramen of
Magendie
d = lateral aperture
of fourth ventricle
Z = central canal of
the spinal cord
In this difference between the flow rate of two fluids we
are able to perceive another function of the CSF. The brain is relieved of the
conditions of gravity and it also opposes the accelerated blood flow with a
circulation of its own that is very much slower. Being present all around the
brain, the CSF ensures the even distribution of the pulsating pressure of the
blood flowing through it, so that we do not feel this pressure. The CSF has
here an equalizing function, spread out over an area, that counteracts the pulsating,
swelling pressure of the brain (turgor). It assists the veins, suppressing the
waves of blood coming from the heart. Without the CSF, the brain would
experience the full power of the strong pulse beat we can feel in the neck.
The hydrostatic function of the CSF that eliminates weight
is a precondition for the other function through which the pulsating movement
of the blood is muted and brought to rest in the head. The one is a specialized
function arising from the other. The function of suppressing the blood is a
special differentiation and a consequence of the loss of weight effected by the
CSF. The function of the CSF relating to the weight of the brain is more of an
outer function; it becomes more of an inner function in relation to the number
of pulse waves which the CSF opposes with its slowness, capturing them and
making them ineffective.
We noted that the circulation of the CSF is maintained by
forces of pressure and of negative pressure or suction. These are the same
forces as the gravity and buoyancy acting on the brain, but in a modified form,
functions of a dynamic circulation.
The configuration of the ventricular system reflects the
growth and development of the brain. The hindbrain grows from front to back in
a circular arc; it comes to overlie the older parts of the brain. Inside the
brain, this anteroposterior movement is reflected in an empty space, a negative
form, and the CSF is secreted into this. From these empirical data arises the
concept of a negative space with suction properties. Inside the brain, we can
see etheric space taking organic form and having an effect on gravity through
the CSF. At the same time we consider the conditions under which thinking is
freed from the forces of growth and from disruptive organic functions: The
forces of the inner negative space become outer ones in the liquor, and in
doing so cancel the property of gravity that belongs to outer matter. The
forces of etheric space need a mediator if they are to act on the mechanics of
the physical and mineral world. The CSF is that mediator, a medium that enters
into both spheres of forces.
This concept of a medium which we have now established can
also be applied to the potentizing tendency in the cranium that was referred to
at the end of Part I of this paper. Matter has mass, like the brain; the
residual weight of the brain indicates that matter can be potentized through
rhythm; its forces are active in the medium, which is analogous to the CSF.
Respiration and the
CSF
The CSF in the vertebral canal is displaced by the
respiratory movements; synchronous with the movements of the lung, the fluid is
pushed up and down and therefore also moves within the water-filled cushion.
There are two basic physiological preconditions for this. Firstly, the veins at
the base of the skull that lie adjacent to the CSF space and the veins of the
thorax and abdomen are all in communication, and a similar communication exists
also between the venous plexuses of the vertebral canal and the CSF in the
vertebral canal.
The second precondition is that the normal venous pressure
is equal to the pressure of the CSF. Any
increase in venous pressure is immediately reflected in the CSF and vice versa.
We have already established that the CSF space is a
sensitive pressure receptor. How can the pressure in the CSF be raised? By
coughing, sneezing, and pressure on the lateral veins in the neck. This causes
congestion in the veins of the neck, and drainage of blood from the brain is
impeded. The blood held back above the compressed veins causes the CSF pressure
in the cranium to rise. The pressure is transferred via the veins of the neck
into the water-filled cushion in the cranium. The same effect is produced by
coughing and sneezing, with the increased respiratory pressure passing right
into the cranium, i.e. passing through the veins and into the cranial CSF.
If a cerebellar tumor obstructs CSF drainage, the CSF is
forced forward by the increased pressure and into the sheath of the optic
nerve. Fundoscopy will show papilloedema at the point of entry of the optic
nerve into the eye. Abdominal muscular pressure can produce a similar effect,
by putting increased pressure on the abdominal veins. The resulting back
pressure of the blood is comparable to that produced by compression of the
veins in the neck, but the route by which the pressure is transferred is much
longer, passing via the veins of the spinal cord, through the vertebral canal,
to the CSF in the cranium.
The foramen magnum acts as a safety valve in this case, for
it is at this point that the spinal fluid that is forced upwards is able to
escape into the cranium. It is also the point where CSF from the cranium can
escape into the vertebral canal.
The foramen magnum is an extremely sensitive valve. If a
spinal puncture is done in a patient with a cerebellar tumor, the flow of fluid
from the needle may cease abruptly.
The tumor and the cerebellum are suddenly pushing the
medulla oblongata into the foramen, breaking the communication between the CSF
in the cranium and the vertebral canal. Pressure of nervous tissue on the bony
margins and surrounding areas causes fatal nerve cell damage in this area,
among other things to the respiratory centre. That is why sudden death may
occur on lumbar puncture if a cerebellar tumor is present. It serves as an
example to demonstrate the important role the CSF plays in maintaining the
nervous system, and what can happen when buoyancy is lost and gravity alone is
taking effect. The effect Hyrtl produced in dogs (Part I of this paper) here
occurs in man due to pathological causes.
Coughing, sneezing and abdominal muscular pressure are only
able to produce those one-sided pressure changes in the CSF because they
increase respiratory pressure. The effect of an inspiration is as follows: As
soon as the diaphragm pushes further down into the abdomen, there is increased
pressure on the abdominal veins, with the result that some of the CSF in the
vertebral canal moves up into the cranium, lifting the brain. The actual
pressure of the cranial CSF begins to increase when the descending diaphragm
reduces the volume of the abdominal cavity. The inspiratory pressure therefore
effects first a reduction in abdominal space, then increased pressure in the
veins of the abdomen, in the CSF in the vertebral canal, and finally in the CSF
in the cranium; the increase in pressure travels along this route like a wave,
finally lifting the brain. Inspiration and expiration may be compared as
follows:
Inspiration Expiration
1) as the diaphragm 1)as the diaphragm
descends, putting pressure ascends, reducing the pressure
on the abdominal veins, on the abdominal veins,
the increased pressure in the veins of the vertebral
the veins is transferred canal and the CSF are
to the vertebral canal; subject
to less pressure,
increased CSF pressure with the result that CSF
drives the fluid through moves down from the cranial
the foramen magnum into space, again through the
the cranium. The brain foramen
magnum. The brain
is lifted forward and
up; moves downward,
following
it follows the upward the
downward movement
movement of the CSF. of
the CSF.
2) The movement of the CSF 2) The movement of the CSF
becomes a reflection of becomes a reflection of
inspiration: As air is expiration: As carbon
dioxide
forced into the lungs, leaves
the lung, so fluid
so fluid is forced into flows from the cranium.
the cranium on inspiration.
As far as I can see, Rudolf Steiner always referred to this
abdominal form of respiration.
With the thoracic form of respiration, conditions are
reversed: inspiration produces a negative pressure in the veins of the neck,
resulting in the brain moving down; expiration causes an increase in pressure,
lifting the brain. A mixed form of respiration would result in a brief thoracic
upbeat, followed by an abdominal main beat. To quote Rudolf Steiner:
"In breathing the air out, we push the diaphragm
upwards. That action is connected with a relief of pressure on the whole
organic system below the diaphragm. As a result, the cerebrospinal fluid in the
skull, in which the brain is floating, is pushed downwards. This cerebrospinal
fluid is nothing but a denser modification, as I should like to put it, of the
air, for it is in truth the exhaled air which causes this. When I inhale again,
the cerebrospinal fluid is pushed upwards, and in my breathing I am constantly
living in this downward and upward movement of the cerebrospinal fluid, a
distinct reflection of the whole respiratory process." (R. Steiner, Nat.
Sc. Course 1920/21, Bibl. No. 320).
The respiration has two functions. One of them is
physiological, the control of oxygen and carbon dioxide as a chemical function.
The other proceeds concurrently, on the basis of the differences in pressure
produced as we inhale oxygen and exhale carbon dioxide. Both are transmitted
through the whole body. The
excursions of the CSF bring an external physical principle into play biologically,
their function being to lift out the organ of thought and to damp down the
pulsation of the blood. That is achieved for the brain, for instance, and for
the closely adjacent senses. Chemically this is reflected also in the
well-known blood-brain barrier existing on the material level, a barrier that
makes it difficult to use therapeutic agents in material form to treat the
brain and nervous system.
Carbon dioxide has a powerful effect on the cerebral vessels
and therefore on the circulation of the brain. 5-7 % of carbon dioxide (CO2) in
the air we breathe cause a 70 % increase in cerebral blood flow. The vessels
dilate, so that more blood is able to pass through them. If the CO2 level
drops, e. g. by increased exhalation, vasoconstriction results, and the
circulatory volume may drop by one third.
If we get a person to inhale pure oxygen, blood flow is cut
down by reflex action; a reduction in oxygen (to 10 % of the air inhaled) will
increase the circulation. The two respiratory gases carbon dioxide and oxygen
thus act as chemical agents; the CSF produces the same effect
"physically", by acting from without — for it is obvious that the
circulation of the brain is subtly changed as the fluid moves up and down. The
respiratory function is thus reflected in the excursions of the CSF, and the
movement of the CSF presents itself as a modified, denser form of respiration. (To be continued)
Literature
D. W. C. Northfield. Surgery
of the Central Nervous System, 1973.
Author’s address: 7302 Ostfildern-Nellingen,
Friedrich-List-Strase 27, W-Germany