(Original title: Ist Himtod gleich Tod? Merkurstab 1994; 47:456-65. English by A. R. Meuss, FIL, MTA.)
Historical evolution
First of all, a definition: "brain death" as total cessation of integrated brain
function, followed by necrosis, has to be clearly distinguished from "locked-
in syndrome" (motor paralysis in all parts of the body, with the patient
sentient and awake, a condition due to interruption of the corticospinal tracts
between midbrain and pons).(1)
Analogous to other organs (renal or liver failure) we should really be
speaking of "cerebral failure" rather than "brain death."
Irreversible loss of all brain function causes spontaneous respiration to
cease, leading to "cardiovascular death." The syndrome has only been
observed with the development of intensive care units. Long-term artificial
respiration has made it possible to keep patients alive: the disease as an
"artefact of intensive care treatment" usually manifests hours, days or a few
weeks after initiating intensive care;(2) and "dying and death have since gained
a new dimension."(3)
In ancient Egyptian medicine the rule was that people were alive for as
long as they breathed; death was near when the heart no longer "spoke,"
when the vessels "fell silent."(4) This has continued to be the generally-
accepted view up to the present century. It is a reflection of human evolution
that the definition of death no longer bases on the heart and respiration but
on brain function.(5) The syndrome was first described in 1959 as coma depasse.(6)
Many definitions were suggested,(7) with "brain death," a most inappropriate
term, finally winning the day. In the field of intensive care medicine, it soon
became necessary to develop guidelines and recommendations as to how
such patients should be considered.
Another new development which affected the issue was transplantation.
The first heterologue attempts (animal to human being) were made between
1906 and 1923. All came to grief on the biologic barrier of immunity. The first
homologue attempts (human to human) were made by Varony in Russia in
1936. Rapid development finally came in 1962/63, following immune-
suppression with azathioprine and corticoids. The first liver was transplanted
in March 1963, the first lungs in June 1963, the first pancreas in 1966,
and the first heart on 3 December 1967.
The cyclosporin era began in 1976/78, effectively controlling rejection
reactions. As early as 1968, the Pittsburgh technique of perfusion cooling of
organs for transplantation had matured to a point where it proved useful."(8,10)
As time went on it became necessary to agree on the possible and legitimate
moment when organs could be removed.
Several sets of criteria for "brain death" were developed, including the
Harvard criteria in 1968, others in England in 1976 and 1979, the USA in 1981,
Switzerland in 1983, and in the Federal German Republic in 1969,1982,1986
and in 1993. The German Medical Association has consistently stated that the
guidelines can only "aid physicians in making their decision" and are not
legally binding.(11,14)
The discussions held over the last two years have shown quite clearly,
however, that cerebral failure is not generally accepted as the moment of
death (with all the consequences, e.g. removal of organs).
An apt exposition of the problem was made in Denmark in 1989:
I. A person is dead when the following have completely and irreversibly
ceased:
1 cardiovascular functions
2 respiratory function
3 cerebral function
II. Cessation of brain function signifies the irreversible beginning of the death process.(15)
Unfortunately this is an isolated instance in the literature.
The current criteria of cerebral failure are essentially based on three
parameters: (morphology (CT), cerebral circulation (angiography, Doppler
ultrasonography, perfusion scintigraphy) and brain function (neurologic
examination: EEG, apnea test).
Pathophysiology
The central nervous system (not so much the spinal cord), "which has no
vitality of its own and needs 'intensive care' to prevent it perishing prema-
turely, is subject to decomposition and decline, atrophy and degeneration,
rigidity and death."(16)
Damage may result from rapid acceleration or deceleration, rotation
trauma, gas bubbles rupturing the capillaries, parenchymal necrosis and
hemorrhage, tissue contusion, neural tract rupture, ischemic lesions and
edema. Intracerebral hematomas may increase in size within hours or days.
A vicious circle evolves with edema leading to hypoxia which, in turn,
increases the edema. Instability of the brain's autoregulatory functions may
result in systemic disorders such as circulatory problems, with poor
oxygenation causing additional damage. Cerebral edema myelophthisis,
known as "edema necrosis," shows in the CT as internal hydrocephalus.
Other factors indicating a poor prognosis include the absence of periodic
sleep patterns in the EEG.(1)
Ischemic damage due to circulatory failure or inadequate resuscitation,
for instance, is biphasic. Initially, when the oxygen supply is interrupted,
serious but not absolutely irreversible damage is caused to the brain. If the
first phase has been too long, the second, post-ischemic phase results in
serious and often irreversible damage. It is the recirculadon phase. Several
factors are involved:
a) Post-ischemic hypotension: acid equivalents are washed out from the
brain, resulting in vasodilatation and a drop in blood pressure. The
hypotension tends to be of extended duration if the cause is cardiac, as heart
and circulation do not resume function immediately. This is the reason for
the much shorter period available for brain revitalization after cardiac
arrest.
b) Disseminated intravascular coagulation develops shortly after onset of
ischemia and is enhanced in the early recirculation phase. Additional
factors are increasing thrombocyte aggregability in the ischemic phase;
serotonin release from aggregated platelets leading to vasoconstriction;
damage to peripheral organs (heart, kidneys, pulmonary shock) may
prevent reoxygenation and increase cerebral edema; changes in blood
viscosity with decreased flow rate and impaired microcirculation.(17)
c) Post-ischemic cerebral edema with increased intracellular osmolality and
loss of membrane potential results in massive electrolyte shifts. Onset of
recirculation causes massive fluid volumes to enter brain tissues,
increasing edema and thus causing a rise in intracranial pressure.
d) Multiple metabolic imbalances develop in addition.
This brief outline shows that circulation may start again after ischemia
but generally ceases again within a short time (a few minutes) if the cerebral
edema has reached a critical level.(18)
Complete cessation of cerebral circulation causes death of the brain as an
organ, with irreversible loss of function. This results in dissociation of the lost
brain function from persisting peripheral organ functions if circulation and
respiration are supported in intensive care (the latter by use of a respirator).
The brain represents only about 3% of the total organism,(19) but loss of
cerebral function has serious consequences for the whole. Cerebral failure
involves the loss of higher brain functions: consciousness, mentation,
perception, and sensory perception. Cranial nerve and brain stem reflexes are
absent (dilation of pupils, fixed pupil, comeal reflex, vestibular reflex, cough
and retching reflexes, no reaction to aspiration). Extensor spasticity
progresses to general loss of muscle tone. The vital functions of the brain
stem are lost: diabetes insipidus, absence of circadian variations in
temperature, blood pressure and, pulse, and of their physiological control.
Metabolic imbalance results from failure of the hypothalamic-pituitary,
and diuretic system.
Extended periods of artificial respiration and other measures may
provoke a wide range of strange, "meaningless" phenomena: profuse sweats
alternating with rubor in some parts of the body, phases of hypo- and
hyperthermia, inexplicable variations in blood pressure and pulse rate that
may come up suddenly and just as suddenly disappear again, extensor
spasms or twitching of muscle groups in the extremities. These phenomena
have no apparent purpose; they are merely reflex movements not controlled
by the ego and lacking in coordination.(20,25)
Anthroposophic aspects
Past, present and future all coexist in the human being. This can be seen in
the biology of the newbom. The neurosensory system is fully developed at
about two months before birth, the rhythmic system reaches maturity at
birth, while the metabolic system and especially the limbs are still in the fetal
stage.
No other newborn beings show this triunity to the same degree as
humans who are born post term in the head, on term in the heart and
respiratory systems, and prematurely in their limbs.(26)
A. Portmann distinguishes three functional regions in the neurosensory
system: the elementary apparatus which controls the simple functions and is
mainly located in the spinal marrow and parts of the extended marrow.
Reflex-type reactions are part of this system.
A second, superior system is the autonomic apparatus. Elementary
functions are combined for the higher functions of metabolism, reproduction,
alternation of sleeping and waking states, hunger and satiety - all the
changes known to us as "moods." This apparatus is located in the my
elencephalon, the hypothalamus, the basal ganglia of the forebrain and in me
splanchnic nervous system.
The somatic apparatus concerns the sphere of the senses and the higher
functions (orientation in space, relationship to the environment). It is the "site
of highest integration," located in the metencephalon, mesencephalon,
hemispheres of the telencephalon with the cerebral cortex.
The elementary and autonomic apparatuses show a high degree of
structural complexity even in the lowest mammals. "This part of the nervous
system shows the fewest differences, relatively speaking, and these
apparatuses are always fully developed at an early ontogenetic stage."(27)
The neurosensory system mainly serves mental activities that take place
in the waking state. "Sensory perception, ideation, memory and thinking are
made conscious by them. Its processes are directed outward and inward, the
impulse being to perceive or rather to convey sensory perceptions."(28)
"The senses have significance not only for the soul, for the creation of an
inner world, not only for maintenance of the body (perceiving ongoing
processes, the state of well-being, the condition of the organs, the activity of
the limbs); they are the places where entities from the earthly and cosmic
periphery enter into the inner human being (or evoke counter reactions from
the inner life)."(28)
The head is an offprint, a kind of elimination of the ego, astral body and
ether body. These three higher aspects of the human organization create their
organ, forming it out fully, and then eliminate it; they are then free, able to
enter and leave again, the organ having become permeable. Here we have the
greatest differentiation, form and plastic principle - organization at the level
of perfection.29 Cerebral failure merely means that the brain is no longer open
to those three higher aspects. The sense organs are almost physical apparatuses,
a gulf "extended into the human being by the outside world."(30)
We deal with the outside world, communicating with it, making our
mark on it and being influenced by it in three areas. In the metabolism this
happens through nutrition; we impose our will on the environment and take
action in it. The things we attempt, desire and do, the unfulfilled seeds of the
will, provide us with the capacities for a future life.
In the rhythmic system we inhale and exhale, and live in the world of
feelings; we live life in the present as we practice and learn.
In the neurosensory system, an imponderable breathing process occurs
between us and the environment, skills, talents and capabilities point to an
earlier life. This imponderable breathing process occurs mainly through the
12 senses(31,32) and plays a role in making human evolution possible and
maintaining it in time.
Failure in each one of these three areas of communication or relation has
its own specific quality and consequences. Paralysis in the sphere of the limbs
makes it more difficult to perform an action: the limb itself becomes outside
world.(33) Paralysis in the metabolic sphere prevents active involvement with
matter so mat the energies normally evolved in the process gradually fade
away. Failure of the rhythmic system - even lack of ability to move in
rhythm, rigidity - is a serious pathological sign and signifies that the present
life will soon be ended.
Lack of external stimuli when organ function is normal clearly indicates
absence of the imponderable breathing process. Without those external
stimuli proper human development is seriously affected - "wolf children"
are a good example. If cerebral function itself ceases, (irreversible failure) the
imponderable breathing process cannot take place consciously. It is then no
longer possible to maintain a fully human existence as the necessary external
stimuli cannot be taken in and digested.
The body-oriented integrative power of the ego organization graduallyweakens.
The organization of the human head and the central nervous
system can no longer perform their function as offprint and have become
impermeable to the ego, astral body and ether body. A dying process ensues.
The brain as the "indispensable intermediary" between environment and
human being is no longer able to perform its function, which is to maintain
the specifically human aspect.(34) Physiologic respiration ceases and is taken
over by a respirator in the case of such a patient. We are thus able to ensure
only one aspect of respiration, which is to supply air and maintain the gas
exchange in the lung.
Form is embodied in the human physical body. It arises from the
twelvefold zodiac.
The breathing life in the etheric fulfills another function, for the breathing
process yields the images of all our internal organs. Images of our organs,
initially immaterial, are created "via the breathing process." Physiologic res-
piration enables the human being to have a share in the form which is created
out of the starry heavens. Those images are inhaled, as it were. They become
reality (including form) as matter is deposited in the images.(35)
The image nature of respiration and the creation of form are seriously
affected by artificial respiration. With the form-creating life taken away, the
individual is no longer able to maintain true humanity by taking hold of it
again and again and giving it shape. Thus the process of dying begins.
In sleep, ego and astral body have separated from the ether and physical
bodies. The human being does not become a plant, however, because the
activities of astral body and ego nature still continue.(33) "Because the ether
body remains connected with the physical body during sleep, vital activities
continue."(36)
The moment the ether body leaves the physical body, disintegration sets
in. Processes of dissolution and autodigestion begin, with the chemical forces
acting the way they do in the outside world. Death ensues, and decom-
position starts. The ether body is then connected with the astral body in the
absence of the physical body. The latter is left to the forces of gravity and
becomes a decomposing corpse in the physical world.
The spirit takes a different path, one that only becomes possible once ego,
astral body and ether body have separated from the physical body. Different
laws then apply: the inner world (thoughts and life of feeling) becomes outer
world, pouring out into the realm of the stars; the outer world of our actions
becomes inner world. We work through the incarnation that has just ended
and prepare for the next.
After death (separation of ego, astral body and ether body) new qualities
emerge that cannot be seen as a linear continuation of life. The characteristics
of life (growth, flow, nutrition, warmth) leave the body, which becomes a
corpse and is left to physical forces such as the force of gravity. Dissolution,
autodigestion, decomposition and decay begin.
Loss of consciousness and self awareness, serious as it may be, does not
signify the death of the individual. Loss of a physical function or of an organ
(there is, of course, a hierarchy of the organs and their functions) cannot be
equated with death of the individual. In a case of renal failure or another
condition resulting in loss of kidney function, we will, of course, initiate
dialysis to allow life to go on. Quite rightly, we do not speak of a "kidney
dead person."
Someone in cerebral failure receiving artificial respiration cannot,
anthroposophically speaking, be called dead. The symptoms described above
make this quite clear. The physical body does not fall into decay. Physio-
logical processes arising from the interaction of physical body and ether body
stimulated by astral body and ego continue; respiration, circulation and
metabolism can also be observed to proceed, with blood pressure, spinal
reflexes and elimination, reflecting astral body activity, still present.
The coordinating function of the ego is usually no longer observable, nor
are higher nerve functions. Consciousness and self awareness have gone.
Hormonal regulation tends to be seriously affected; purposeful processes are
no longer possible, and "meaningless" reaction patterns appear.
Part of the gesture and character of death is the irreversible separation of
functions into disintegrating individual parts and absence of coordinated
activity, with centrifugal forces dominant. The situation is one of multiple
organ failure. The life-maintaining centripetal, centered principle is an ego-
controlled gesture.
With cerebral failure, centrifugal forces gradually make their appearance.
Tendencies of dissolution, of weakening, develop that point to a slow dying
process. We do not diagnose cerebral failure and then decide what treatment
is necessary. Instead we must undertake the treatment of a seriously ill
individual, often unable to prevent cerebral failure in the process.
Intensive care offers the opportunity - and we are obliged to take it - to
maintain incarnation. It is not in our power to prevent death. Irreversible
cerebral failure thus is a serious condition which rapidly leads to death in the
above sense unless help is given from outside. Intensive care allows us to
intervene from outside and maintain life for a time. Cerebral failure (with
treatment given) marks the beginning of a dying process. Anthroposoph-
ically speaking, this cannot, however, be equated with death nor with a state
of consciousness similar to deep sleep.
The brain and spinal cord are given maximum protection from the
outside world by their bony integument. The spinal marrow must be con-
sidered to be an organ that has remained at an earlier stage of evolution, a
bone marrow of me first order - the brain being bone marrow of the second
order - "...a metamorphosed earlier bone marrow... that has been such in the
past but has been metamorphosed into the brain."(37 )The brain is the
"instrument" for higher soul activities. These are "guided" by the brain. It is the
place were we create our "thought-out ideas." There human beings do not act
by means of reflex movements but reflect on things, and in this sense the
brain is the instrument of inner activity. Reflex movements are compulsive
by nature (a stimulus evokes a movement response without our thinking
about it), and there we see the activity of me spinal marrow.
In dream life, with daytime waking consciousness gone, images appear
on the horizon that have the same direct necessity. They arise compulsively,
without our conscious doing, like reflex reactions in the waking state that
result in movements, but retain their image character.
"Occult investigation shows that a mysterious spinal marrow exists in
the brain which is the instrument of dream life." This spinal marrow becomes
active "when people are asleep and dreaming. Its activity is then of a kind
appropriate for a spinal marrow, arising from necessity"(37)
In cerebral failure, "reflex-type" movements occur that are spinal in
origin but generally arise without stimulus, and seemingly without reason -
a caricature of a dream?
Ego and astral body are archetypal images and as such spiritual. Blood
system and nervous system are images of them. The ether body, on the other
hand, takes its orientation more from the physical body.
On the one hand, the blood presents itself to me outside world rather like
a writing tablet; on the other, it exists for the inner world. The ego also has
two aspects. It lakes up impressions of the outside world, and it can also be
given up to an inner world. Impressions are inscribed in the blood via the
nerves.
"In ordinary life, as it generally goes, the process is such that an effect
transmitted via the nerve inserts itself in the blood as though on a writing
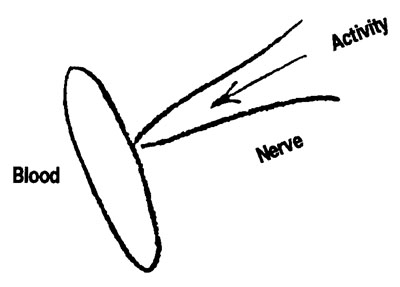
tablet and has, thus, inscribed itself in the instrument of the ego.(37) Inner
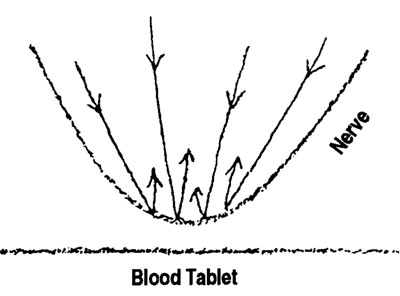
feelings and ideas, which should be higher, "moral or intellectual ideas,"
extreme inner concentration, engage the nerve, which is withdrawn from the
blood, as it were.
"Contents of the conscious mind are primarily taken hold of by the
nerve, thus separating nerve activity from blood activity." The nerve is
released from connection with the blood; the activities of the nervous system
become retrograde, as it were. "The ego is consciously lifted out of the astral
body's sphere of action."(37) At the nerve ends, we rebound and "life goes out
in the world beyond the senses."
This is the occult physiological process of conscious spiritual training.
Spiritual training involves a temporary, occult physiological separation of
nerve and blood which is deliberately induced in inner exercise.
Cerebral failure thus marks the beginning of a dying process, with the
individual on the threshold. In spiritual terms, the connection between sense
organ and blood is broken at the distant periphery. This is the irreversible,
physically pathologic caricature of conscious spiritual training.
References
1 Poeck K. Neumltyie Springer 1982.
2
Kriterien des Himtodes (brain death criteria). Deutsches Aerzteblatt 1982; Heft 14, April.
3
Pia HW. Himtod (brain death). Deutsches Aerzleblat 1986; Heft 31/32,1 August.
4
Lichtenthaeler. Cescfachte der Median (history of medicine). Aerzteverlag 1982.
5
Steiner R. AnHwposophical Leading Thoughts (GA 26). Tr. G. & M. Adams. London: Rudolf
Steiner Press 1973.
6
Moolaret P, GoulonM. La coma depasse. RevNeurol 1959; 101.
7
Pohlmann-Eden B. Die Hirntoddiagnose: Begriffsbestimmung - klinische Kriterien
(diagnosis of brain death: definition of terms - clinical criteria). Zschr Transplantationsinedizin
1992;140.
8
Kuess R, Bourget P. An illustrated history of organ transplantation. Sandoz.
9 Starzl TE. Die Entwicklung der Ganzorgan-Transplantation. Sandoz-Bulletin 23,1987.
10
Reichart B. Herz-und Herz-Lungen-Transplantation. Schuiz Verlag 1987.
11 Kriterien des Himtodes (brain death criteria). Deutsches Aerzteblatt 1986; Heft 43, October.
12 Kriterien des Himtodes (brain death criteria). Deutsches Aerzteblatt 1991; Heft 49, December.
13
Birnbacher D, et al. Der vollstaendige und endgueltige Ausfall der Hirntaetigkeit als
Todeszeichen des Menschen (complete and final cessation of brain activity as a sign of death).
Deutsches Aerzteblatt 1993; Heft 44
, November.
14
Haput WF, et al. Die Feststellung des Todes durch den irreversiblen Ausfall des gesamten
Gehims (establishing death due to irreversible cessation of all brain activity). Deutsches
Aerzteblatt 1993; Heft 45, November.
15 Danish Council of Ethics. Death Criteria: a report. Copenhagen 1989.
16
Treichler M. Sprechstunde Psychotherapy (psychotherapy in practice). Urachhaus 1993.
17
Bavastro P. Die Mila-ozirkulation. I) DerMerkwstab 1990 Heft 6; II) Der Merkurstab 1991 Heft1.
18
Hossmann KH. Experimentelle Crundlagen der Reanimation des Hirnes nach
Kreislaufstillstand (exp. bases of brain revitalization after circulatory failure). Das Gehim und
seine Erkrankungen Band 1. Medicinale XVII. Iserlohn 1987.
19
Linke D. Klinische Neurohiologie. Himtod und Schwangerschaft (brain death and pregnancy).
Enke Verlag 1993.
20
Harrisson. Prmapien der Inneren Medizin. Schwabe 1989.
21
Angstwurm H. Himtod und Organexplantation (brain death and organ explantation). hi
Dickganz/Brandt Therapie und Verlaufneurologischer Erkrankungen 1989.
22
Schuster HW. Intensiv-Medizin. Thieme 1989.
23
Lawin P. Praxis der Intensiv-Behamttung. Thieme 1989.
24
von Reutem GM. Zerebraler ZirkulationsstiUstand (cerebral circulatory failure). Deutsches
Aerzteblatt 1991; Heft 49.
25
Hacke. Neurologische Intensivmedizin. 1986.
26 Das
Schicksal manipulieren? (manipulate destiny?) Freies Geistesleben 1986.
27
Portmarm A. Einjuehrung in die vergleichende Morphologic der Wirbeltiere (intro. to comparative
morphology of vertebrates). Schwabe 1983.
28
Sieweke H. Cesundhdt und Krankheit als Verwirldichungsfonnen menschlichen Daseins (health and disease as forms of human existence). Philosophisch-Anthroposophischer Verlag am
Goetheanum 1967.
29 Steiner R
. The Spiritual-Scientific Aspect of Therapy (GA 313). Lecture of 11 April 1921. Tr. R. Mansell. Long Beach CA: Rudolf Steiner Research Foundation 1990.
30 Steiner R. Spiritual Science and Medicine (GA 312). Lecture of 3 April 1920. Tr. not known
.
London: Rudolf Steiner Press 1975.
31
Knobel H. Ich-Gestalt und Sinnenlehre (ego configuration and theory of the senses). Zbinden
Verlag 1984.32 Lauer HE. Die zwodf Sinne des Menschen (12 senses). Novalis Verlag 1977.
33
Steiner R, Wegman I. Fundamentals of Therapy (GA 27). Tr. E. Frommer, J. Josephson- London: Rudolf Steiner Press 1983.
34
Uexkuell T. Psyche and Soma. In Das Cehirn und seine Erkrankungen (the brain and its pathology) (II) Band I. Iserlohrc Medice Hausdruck 1988.
35 Steiner
R. Anthroposophie als Kosmosophie Teil n (GA 208). Not translated.
36 Steiner R. Occult Science 197 An Outline (GA 13). Chapter on sleep and death
. Tr. G. & M. Adams. London: Rudolf Steiner Press 1962.
37 Steiner R. An Occult Physiology (GA 128). 1st and 2nd lectures. Tr. E. Frommer. London: Rudolf Steiner Press 1983.
38 Editorial: Brain death and live birth
. JAMA 1982; 248:1101.
39
Dillin WP, et al. Life Support and Maternal Brain Death During Pregnancy. JAMA 1982; 248: 1089.
40 Field
DR, et al. Maternal Brain Death during Pregnancy. JAMA 1988; 260: 816.
41 Bernstein
IM, et al. Maternal Brain Death and Prolonged Fetal Survival. Ohstet e Cynecol 1989; 74:434.
42
Loewy EH. The Pregnant Brain Dead and the Fetus: Must we always try to wrest life from
death? Am ] Obstet Gynecol 1987; 157:1097.
43
Piechowiak H. Der muetterliche Himtod am Ende des zweiten Trimenons (maternal brain
death at end of 2nd trimester). Schweiz Rundschau Med 1984; 74:261.
44
Pichowiak H. Von einer Toten geboren (bom of a dead woman). Fortschr Med 1986; 104:56.
45
Haikkinen )E, et al. Life support for 10 weeks with successful fetal outcome after maternal
brain damage. Br Med J 1985; 290:1237.
46 Sampson MB, et al. Post-traumatic Coma During Pregnancy. Ohstet e Cynecol 1979; 53:
Nr. 3
(supplement).
47
Shrader D. On Dying More than One Death. Hertmgs Center Report Feb. 1986.
48
Nuutinen LS, et al. Nutrition during Ten-Week Life Support with Successful Fetal Outcome
in a Case with Fetal Maternal Brain Damage. J Parenferal and Enteral Nutrition 1989; 13:432.